Nagaveni NB1*, Shwetha Santhosh2, Matheen Sharif2, Nikhil NM2
1Professor, Department of Pediatric and Preventive Dentistry, College of Dental Sciences, Davangere, Karnataka, India
2Post-Graduate Student, Department of Pediatric and Preventive Dentistry, College of Dental Sciences, Davangere, Karnataka, India
*Correspondence: Nagaveni NB, Professor, Department of Pediatric and Preventive Dentistry, College of Dental Sciences, Davangere, Karnataka, India. Email: nagavenianurag@gmail.com
Received: 25 Nov, 2025 Accepted: 20 Dec, 2025; Published: 03 Jan, 2026.
Citation: Nagaveni NB, Shwetha Santhosh, Matheen Shariff, Nikhil NM. “A Pioneer Case Report on Occurrence of Multiple Tooth Morphological Oddities.” J Oral Dis Treat (2026):111. DOI: 10.59462/JODT.3.1.111
Copyright: ©© 2026 Nagaveni NB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribu tion, and reproduction in any medium, provided the original author and source are credited.
Abstract
Development of supernumerary/accessory roots is a disturbance occurring during formation of hertwig’s epithelial root sheath. The supernumerary roots are most commonly seen in mandibular or maxillary molars referred by ‘radix entomolaris,’ ‘radix paramolaris,’ radix mesio-lingualis or radix disto-lingualis. Mandibular first premolar is tagged as ‘Endodontist enigma’ as it shows astonishing morphological variations in root form or canals. Occurrence of combined compound and complex odontoma in the mandibular arch itself is extremely rare phenomenon. Transmigration of mandibular canine representing an uncommon eruption pattern is also a rare condition. Literature shows occurrence of above-mentioned dental morphological aberrations as an isolated entity. Concomitant occurrence of all these anomalies in a single, normal individual with absence of any systemic, metabolic or syndromic diseases is an extremely rarest scenario not reported till date. Hence, aim of this research article is to describe in detail about the presence of different dental anomalies such as mandibular combined compound and complex odontoma, two-rooted mandibular first premolar and impacted, transmigrated mandibular canine in a non-syndromic patient.
Keywords: Bifurcated premolar, Canine impaction, Mandibular odontoma, Non-syndromic patient, Retained primary teeth
Introduction
Numerous dental anomalies/morphological oddities involving crown or root part of a tooth can occur in human being representing developmental disturbance during dental organogenesis. The morphological oddities may involve the shape, number, size, structure or composition of the tooth, or eruption process of the tooth in an individual [1-3]. Odontomas are the benign odontogenic tumors of epithelial and mesenchymal origin, but now considered as hamartomas lesions. They are a developmental defect of hard dental tissues, referred as benign, tumor-like odontogenic lesions and constitute about 22% of all the odontogenic tumors of the jaw [4]. A pioneer author Paul Broca in 1866 derived the terminology ‘odontome’ and defined it as a ‘tumor formed by overgrowth or transitory of complete dental tissue’ [5]. They are non-aggressive, slow-growing and asymptomatic in nature and consist of enamel, dentin, cementum and varying amounts of pulp tissue. Odontomas are basically classified into two types as compound and complex odontomas [6]. Based on morphology compound odontoma is further categorized into three types as particulate, denticular and denticulo-particulate odontomas [7]. Detailed description of different types of odontomas described by different authors is mentioned in Table 1. Occurrence of both compound and complex odontomas in a single individual is an uncommon instance as the published reports showed occurrence of either compound or complex type [8,9].
Mandibular premolars have attracted academic researchers and dental practitioners for showing aberrant anatomy pertaining to either crown or root portion [10,11]. Premolars show surprising variations in root numbers and canal morphology. A two-rooted mandibular first premolar is a tooth with a rare but documented anatomical variation where it divides into two roots instead of the typical single root posing a most challenging tooth for root canal treatment [11]. Understanding the root number canal anatomy is important before initiating endodontic treatment. Any missed canal or root number will result in treatment failure. As success of root canal therapy is dependent upon a thorough knowledge of the root and root canal anatomy as it helps clinicians to locate all the canals followed by proper cleaning, shaping and obturation of the canal spaces from all dimensions [12,13]. Hence, a great researcher Slowey [12] referred ‘mandibular first premolars’ as ‘Endodontist’s Enigma’ as this tooth is more anatomically surprising by displaying a wide spectrum of morphological peculiarities and may present the greatest difficulty of all teeth to perform successful endodontic treatment. The reason for this is that they are anatomically unpredictable, and often exhibit with a wide variety of morphological rarities. One such morphological oddity is the presence of two roots, with a reported incidence of 1.8%. The difficulties for clinicians are further compounded by the propensities for abnormal variations, narrow mesiodistal dimensions and the resulting restricted access to canals, lack of vision, and presence of apical third trifurcations and deltas [14-15].
Eruption of the mandibular permanent canine happens at the age of 12 to 14 years. Over-retention of primary teeth always give a clue about hidden pathology [16]. Mandibular canines are most commonly get impacted and remain within the bone. Surprisingly the impacted canines instead of being in their position, tend to move towards midline and sometimes cross the midline. Such dental phenomenon is referred as ‘tooth transmigration’ in the dental literature [17]. Therefore, transmigration is characterized by ‘interosseous migration of the impacted tooth crossing the dental midline and seen opposite side of the dental arch.’ Transmigration most commonly affects mandibular permanent canines, can be unilateral or bilateral with no gender predilection [18] The exact etiology behind tooth movement towards dental midline is not known. Presence of transmigration of canine always found with over-retention of the primary canine, or missing of the permanent canine. Most of the transmigrated canines are asymptomatic and hence, they are incidentally detected on routine radiological examination [19].
There are reports showing individual cases involving either crown or root morphological oddities [1- 19]. Occurrence of both crown and root anomalies pertaining to different dental developmental phenomenon is an uncommon finding. Therefore, main objective of the current research paper is to provide a detailed insight on occurrence of multiple aberrant dental anomalies such as complex and compound odontomas, over-retention of the primary canine, transmigration of permanent canine and bifurcated mandibular first premolar. All these tooth disturbances occurred in a normal, non-syndromic 18-year-old male patient. Extensive review of the literature revealed publication of isolated dental entity. Occurrence of above-mentioned multiple tooth malformations in a single patient is not reported till date. Therefore, the present case is the pioneer report show-casing an extremely uncommon rarity.
| Odontoma Types | Description |
|---|---|
| WHO classification [6] Compound odontoma |
Presents as an aberration consisting of all types of dental tissues. Shows an orderly distribution in the form of tooth-like structures. |
| They are predominantly found in the areas of upper incisors and canines followed by postero-inferior regions. | |
| Radiographically, they exhibit an ill-defined radiopaque image made up of multiple radiopacities called denticles. | |
| It is further classified into three types as mentioned below: | |
| A. Denticular – It has two or more separate denticles, each resembling a tooth. B. Particulate – It has two or more separate masses of particles of dental tissues abnormally arranged. C. Denticulo-particulate – It has denticles and particles present side by side. |
|
| Complex odontoma | Presents as an aberration in which some or all dental tissues are present but arranged in a disorganized manner. |
| More commonly observed in the region of the second and third mandibular molars. | |
| Radiographically, these show a non-specific radiopacity with irregular, single or multiple disorganized masses. | |
| Junquera etal lassification [22] | 1. Central (Intraosseous) odontoma |
| 2. Peripheral (extraosseous or soft tissue)odontoma | |
| 3. Erupted odontoma |
Table 1:Different Classification of Dental Odontomas based on Morphology
Case Details
A 18-year-old male patient reported to the Department of Pediatric and Preventive Dentistry, College of Dental Sciences, Davangere, Karnataka, India complaining of dislodged restoration from upper front tooth. Patient was moderately built, well-nourished and did not exhibit any symptoms of systemic, syndromic or metabolic disorders. Patient past history revealed history of dental trauma at the age of 11 years followed by root canal treatment and crown placement for his upper both central incisors. From then patient did not visit dentist and now visited seeking treatment for his dislodged crown. Intraoral examination showed patient with complete permanent dentition except for the presence of retained 73. Permanent 33 was clinically missing. 73 exhibited some degree of mobility. To know the condition of 73 patient was subjected to radio-visuographic examination which revealed presence of small irregular shaped radiopaque masses below the root of 73 and in place of permanent left canine (Figure 1). Radiographic mass exhibited 3-4 small, tooth shaped structures resembling supernumerary teeth (Figure 1). Above these structures, a solitary, small, round shaped radiopaque structure was observed. Regarding root of 73, it exhibited apical one third of root resorption. In addition to these, radiograph also showed half picture of impacted tooth located between right and left central incisors. Hence, to have the complete image of the impacted canine, orthopantomography was taken. Examination of OPG showed rotated and vertically oriented impacted mandibular left canine, its long axis crossing the dental midline. The impacted canine was located below and between roots of two central incisors. Further evaluation of the radiograph showed presence of a supernumerary root in mandibular right first premolar. The two roots were mesial and distally located (Figure 2). Contralateral premolars had single roots. The root of the permanent mandibular right canine exhibited root flexion and aberrant morphology of the root canal Details of morphological oddities are explained in Table 2. No other dental findings were observed. To attend chief complaint of the patient, crown was re-cemented and patient was explained about the existing dental anomalies in his jaw. As all three dental anomalies were asymptomatic, not associated with any pathologic changes periodic observation was advised.
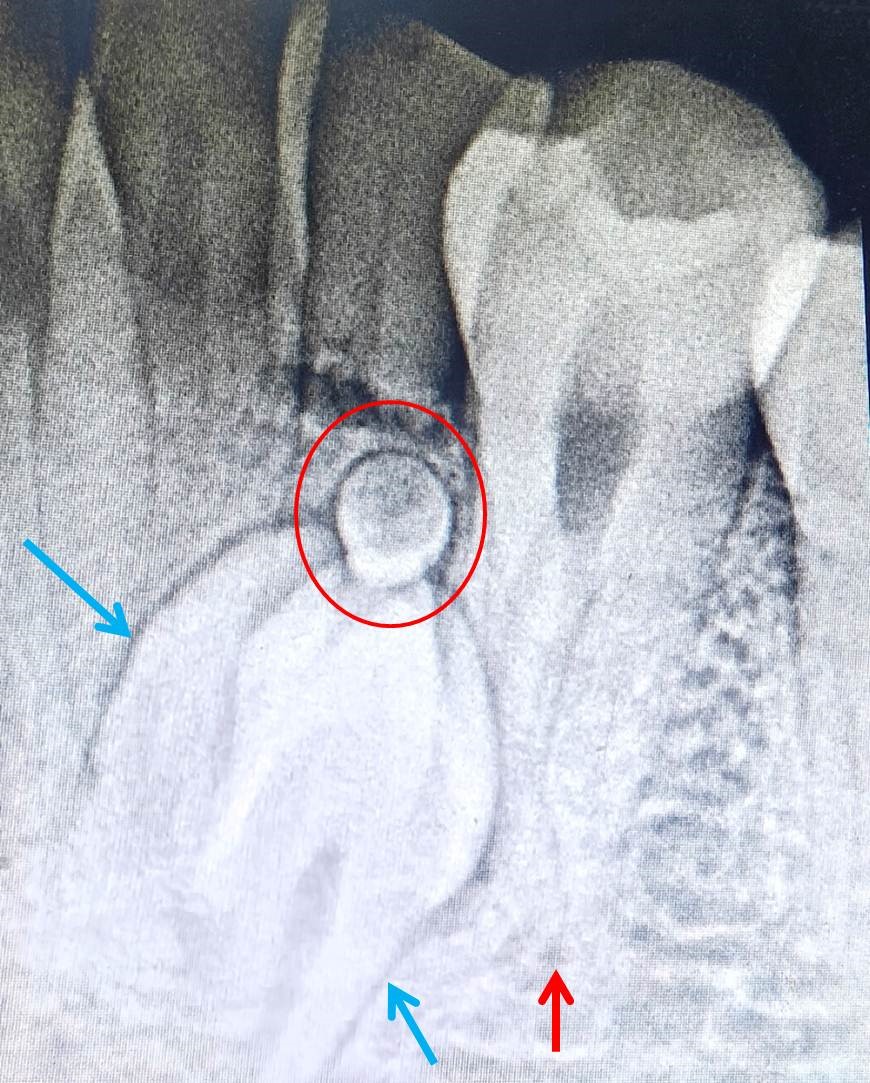
Figure 1: RVG showing combined compound (blue arrows) and complex odontoma (red circle). First premolar with two roots is also evident (red arrow).
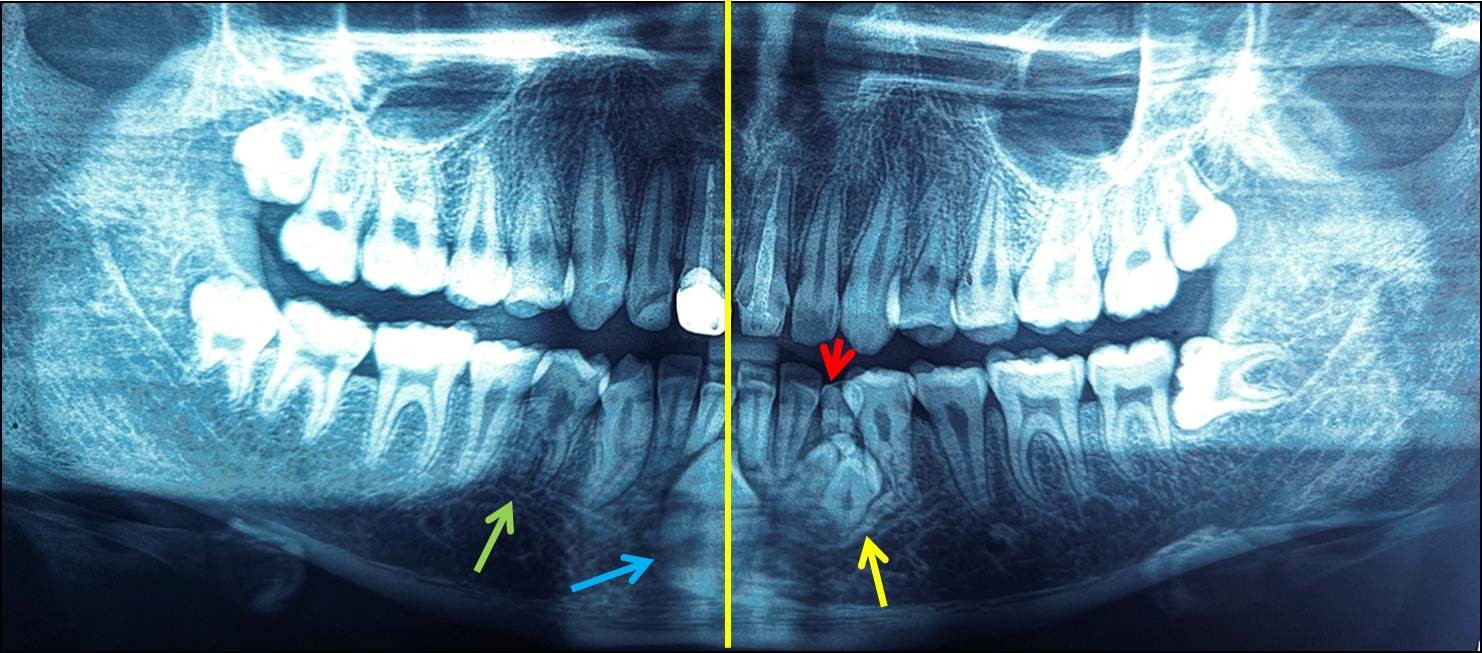
Figure 2:Panoramic radiograph showing bifurcated roots with 34 and 44 (green arrow), transmigrated 33 (blue arrow) crossing midline (yellow line) and impacted combined complex and compound odontome (yellow arrow). Retained 73 is also evident.
| Patient Details | Multiple Morphological Dental Aberrations | ||
|---|---|---|---|
| 18 years Male | Combined compound + Complex Odontome | Transmigrated Canine | Two-rooted mandibular first premolars (Tome’s Root) |
| Asymptomatic Over-retained primary canine | Asymptomatic Over-retained primary canine | Asymptomatic | |
| Radiographic Findings | Impacted radiopaque small, three tooth-like structures observed. Above these structures, a round mass of radiopaque structure was evident. | Impacted permanent left canine was noticed located below the roots of mandibular central incisors. | Bifurcated roots located mesially and distally observed in 33 and 43. |
| Classification Name | Combined compound and complex odontoma (WHO Classification) [6] |
Type 5 Transmigration (Mupparapu Classification) [26] |
Tome’s Root with mesial and distal root (Scott and Turner) [14] |
Table 2:Description of Multiple Tooth Morphological Oddities Found in a Patient
Discussion
Radiographically odontomas exhibit a well-defined radiopacity surrounded by a radiolucent halo in the bone, typically surrounded by a thin sclerotic line. Three developmental stages of odontomas have been identified by researchers [20,21]. The first stage shows radiolucency; second stage depicts partial calcification and the third stage exhibit tissue calcifications predominantly found with the adjacent radiolucent halo. Exact etiology about development of odontomas is not clear. Literature explained infection, genetic factors and local trauma as possible causative factors [22]. It is also stated that failure in organization of odontogenic cells to reach the normal stage of morpho-differentiation, the enamel and dentin tissues are laid down in an aberrant manner. Therefore, because of this reason, odontomas are considered as developmental anomalies rather than true neoplasm [20]. Odontomas are asymptomatic and rarely grow in size. Hence, they are detected following a routine radiological examination. However, infection, swelling, regional lymphadenopathies and pain have been reported in some reports [22]. They are documented more frequently in second and third decades of life. Even in the present case, patient age was 18 years which found in agreement with the reported cases. Occurrence of odontomas is more common in permanent dentition compared to primary dentition. Both types of odontomas occurred most frequently on the right side of the jaw compared to the left side. In contrast to this statement, in the present case, odontoma occurred on the left side of the jaw.
Reports showing occurrence of combined complex and compound odontoma within the same patient are very few. Ahuja et al [4] reported occurrence of impacted, combined compound-complex odontoma located in the mandibular premolar region associated with an impacted second premolar in a 13-yearold female patient. Presence of odontoma caused disturbance in the second premolar eruption leading to impaction of the premolar. Authors successfully removed both odontomas using surgical intervention. Following 6-months of post-operative period, the second premolar erupted normally to reach its position in the dental arch. In the current case three small tooth like structures representing compound odontoma along with small round mass resembling complex odontoma was observed in the left side of the mandible impacted in the place of permanent canine. Based on WHO classification [6], compound odontoma was considered as denticular type. According to Junquera et al classification [23], the present case was classified as central or introsseous odontoma. The permanent canine was impacted and transmigrated towards dental midline and found below and between the roots of two central incisors.
While treating any tooth endodontically, a clinician must always keep in mind about the anatomical variations especially extra canals and roots [24]. In a study performed at University of Washington, the mandibular first premolar exhibited the highest failure rate of 11% [11]. Scott and Turner [13] described the accessory root of mandibular first premolar as Tome’s root. They noted that the form of roots varied through ethnic groups. Prevalence rates of ethnic differences of root morphology reported the highest incidence of more than 25% of accessory roots in Australian and sub-Saharan African populations [13]. The lowest incidence of Tome’s root (0-10%) occurred in Arctic, New Guinea, Jomon, Western Eurasian and American populations. Regarding gender differences in canal morphology, Sert and Bayrili [14] documented higher incidence of 44% of supernumerary roots and canals in females compared to males (34%). A Chinese study [25] found 120 cases of two-rooted mandibular first premolars among 2015 cases, with a total number of 159 teeth using periapical radiographs. According to number of teeth the overall incidence of double roots observed was 4% (159/3972).
The root canal system of premolars with two roots and three canals is typically characterized by one large lingual canal and two smaller mesiobuccal and distobuccal canals in the buccal root [25]. In the present case, first premolar had two roots one was mesial and other distal root. Due to asymptomatic nature, no treatment was indicated and hence the number of root canals could not be assessed. Successful outcome of root canal treatment in premolars with two roots depends upon careful utilization of newer diagnostic aids to locate and treat the entire root canal system. When conventional imaging techniques are used, careful interpretation of angled radiographs is essential to locate presence of extra roots [25]. There are numerous methods for locating hidden canals and their associated root system, including magnification and illumination, radiographic diagnosis, and various other tests like the Champagne bubble test, Redline test, White line test and use of different dyes. Recently CBCT is emerging as a novel and valuable diagnostic aid in studying the variations of root and root canal system [15].
The credit of studying transmigrated canines and framing classification system goes to a great researcher Mupparapu [26]. He classified transmigrated canine into five types based on orientation of the transmigrated canine with dental midline and it is given only for mandibular canine (Table 3) [26]. Based on this classification, the transmigrated mandibular left canine in the present case was categorized as Type 5 as the impacted canine was positioned vertically at the midline below the roots of two central incisors with its long axis crossing the midline. There are drawbacks pointed out by other researchers in Mupparapu’s classification such as bilateral occurrence of canine transmigration is not taken into consideration [17,18]. Hence, a recent study formulated a new classification system (MBS) classification which classified transmigrated canines into main five types with further subdivisions based on several criteria like the distance travelled by the transmigrated canine, unilateral or bilateral occurrence and the axial angulation of the canine with the dental midline [27]. Precise classification of mandibular canine transmigration helps in planning appropriate treatment protocol. In this case, as the transmigrated canine was asymptomatic and located below and between the roots of two central incisors no treatment was performed and only periodic observation was suggested. In the present case, presence of odontoma perfectly indicates the exact etiology for the transmigration of permanent canine. Moreover, over-retained primary tooth also clearly indicates the possibility of impaction of the permanent canine and also indicates the presence of hidden dental pathology [19].
| Types | Description |
|---|---|
| Type 1 | The canine is impacted in a mesio-angular position, with its crown crossing the midline, either labially or lingually to the incisors. |
| Type 2 | The canine is impacted horizontally below the apices of the incisors, near the inferior border of the mandible. |
| Type 3 | The canine is erupting either to the mesial or the distal side of the opposing canine. |
| Type 4 | The canine is impacted horizontally near the inferior border of the mandible, situated below the apices of the opposing premolars or molars. |
| Type 5 | The canine is positioned vertically at the midline, but its long axis crosses the midline. |
Table 3:Classification of Mandibular Canine Transmigration Given by Mupparapu [26]
Transmigrated mandibular canines usually found asymptomatic and hence not detected unless subjected to radiographic examination. Hence the prevalence studies showing true incidence of canine transmigration among different population are very few as it requires unnecessary radiographic imaging. Those few studies which documented the prevalence rates have collected the retrospective radiographic data of the patients’ using radiographs performed for other dental purpose [26]. In the present case too, transmigrated mandibular left canine was detected on incidental radiographic examination. Compared to migration of canine, transmigration refers to is pre-eruptive movement of the tooth across the midline. Maxillary canines rarely show transmigration although they are impacted 20 times more compared to the mandibular canines [17,18]. Panoramic radiographs are essential tool for identification of tooth transmigration. Recently an advanced image technique like CBCT provides more precise diagnosis as it gives complete picture of the transmigrated tooth and its condition like its exact location, relation with adjacent roots, resorption, calcific metamorphosis, bony ankylosis and adjacent vital anatomic structures [15]. Three-dimensional imaging of transmigrated canine is essential when it becomes symptomatic and associated with any cysts or tumor formation or causing bone erosion as it requires surgical removal in such cases [15]. Sometimes transmigrated canines appear at the lower border of the mandible in close proximity with mandibular canal or foramen and mental foramen. Therefore, it is essential to study such teeth in detail during surgical removal or orthodontic movement of the tooth 15]. If the transmigrated canine is impinging on the mandibular nerve, it causes neurologic complications in a patient. Hence, periodic observation of the transmigrated canine is required to avoid complicated future sequel. In the present case, the transmigrated mandibular left canine found asymptomatic although it was located below and between the root of two central incisors.
A peculiar clinical finding exhibited with impacted and transmigrated canines is over-retention of the primary teeth or clinical missing of permanent tooth [19]. When a pediatric dentist encounters such instance, patient should be subjected to thorough radiographic survey to rule out tooth impaction or transmigration. Therefore, it is always better to evaluate the patient between 8 and 14 years during the eruption time of mandibular canine and it is also required to check for the timely exfoliation of the primary canine [19]. This clinical protocol helps in suspecting an impaction and transmigration of tooth and its appropriate diagnosis and timely treatment. The similar observation was noticed in the present case, where the primary mandibular left canine was still stable and overretained at the age of 18 years clearly indicating some hidden dental pathology. Survival status of the over-retained primary tooth most of the time depends on presence of underlying permanent successor. If the permanent successor is congenitally missing, the retained primary tooth survives stable for long time as the root resorption is slow in such cases [16]. Moreover, there are reports showing retention of primary tooth at the age of 55 to 60 years [16,19]. In the current case, even at the age of 18 years, root resorption of only apical third of the root was observed with mild mobility Moreover, presence of primary teeth surpassing its exfoliation time was the main reason in this case which made authors to go for detailed radiological examination. Surprisingly authors found multiple asymptomatic hidden dental anomalies such as combined compound and complex odontoma, transmigrated left canine and first premolar with mesio-distal roots which helped patient to go for early intervention of those anomalies. Treatment of over-retained primary tooth depends on many factors like the condition of the tooth, presence of underlying permanent successor and age of the patient. If the retained primary tooth is stable only wait and watch protocol is helpful [16,19]. When the retained primary tooth shows mobility or root resorption, extraction followed by placement of implants is the suggested choice of treatment. If the underlying permanent tooth is found in favourable position, removal of primary tooth followed by orthodontic movement is essential [16,19]. In the present case, as the retained primary tooth showed apical third root resorption, moderate degree of mobility with underlying dental pathology, a treatment plan consisting of extraction of the retained primary tooth and surgical removal of odontomas under local anaesthesia was planned.
Conclusion
Every dental professional come across numerous dental aberrations while treating children in daily clinical practice. Presence of dental morphological oddities challenges a clinician pertaining to its detection, diagnosis, classification and treatment strategies as these vary from case to case and also differ in each anomaly. The suggested treatment plan given in literature may not be applicable for all cases as treatment plan depends on several factors. Therefore, thorough understanding and detailed knowledge about occurrence of different dental malformations is highly warranted among dental professionals to provide holistic optimal dental care for every patient
References