Mawuli Kotope Gyakobo1*, Alexander Adjei2, Fidelia Akpene Dake3 and Olivia Agyekumwaa Boateng4
1University of Cape Coast, School of Medical Sciences, Department of Internal Medicine and Therapeutics, Ghana
2Shai Osu-Doku District Hospital/Dodowa Health Research Centre, Dodowa, Ghana
3Regional Institute for Population Studies, University of Ghana, Ghana
4Food and Drug Authority, Ghana
*Correspondence: Mawuli Kotope Gyakobo, University of Cape Coast, School of Medical Sciences, Department of Internal Medicine and Therapeutics, Ghana. E-mail: mawuli.gyakobo@ucc.edu.gh
Received: 03 October, 2024; Accepted: 27 November, 2024; Published: 04 December, 2024
Citation: Gyakobo Mawuli Kotope, Adjei Alexander, Dake Fidelia Akpene and Boateng Olivia Agyekumwaa. “Availability and Distribution of Pain Medications in Ghana.” J Fam Med Clin Res (2024): 105.
DOI: 10.59462/ JFMCR.1.1.105.
Copyright: © 2024 Gyakobo MK. This is an open-ac cess article distributed under the terms of the Cre ative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Pain remains one of the major reasons for medical consultations globally and is among the foremost factors of over-the-counter treatment in Ghana. Studies around the world have consistently shown that all types of acute or chronic pain are routinely under-treated. One of the reasons ascribed to this is the scarcity of opioid and other pain medications across the various levels of health care facilities in developing countries. This paper evaluates the availability and distribution of opioid and other pain medications in Ghana.
Methodology: A cross sectional survey was conducted to evaluate the availability of opioid and other pain medications by reviewing records from health facilities at all levels of care including private pharmacies between April to June 2015. This picture has remained largely unchanged. A total of 195 health facilities were randomly selected and reviewed through a structured questionnaire.
Results: Non-steroidal anti-inflammatory agents were the most available and prescribed pain medications (86%), while just over a quarter of health facilities prescribed opioids (27%) and opioids in combination with other pain medications (17%). Regional hospitals recorded the highest availability of pain medications followed by district hospitals while almost none were available in maternity homes. Some of the reasons given for not stocking key pain medications were low demand from patients, prescriber restrictions at the various levels of care and complex disposal regulations.
Conclusion: Opioid medications are not readily available in most health facilities and this has repercussions on the effective management of moderate to severe pain.
Keywords
Pain medicines • Availability • Distribution (Pain medicine, Accessibility)
Introduction
Chronic pain is among the most common causes of morbidity and disability worldwide and significantly associated with chronic diseases like cancer and HIV/AIDS [1]. It also remains the most compelling reason for health seeking and medical consultations globally [2,3]. Pain can also significantly impact the quality of life through its effect on loss of strength, reduced mobility and can interfere with a person’s ability to eat, concentrate, sleep, or interact with others [4]. The effects of pain whether physical or psychological can significantly influence the progression of diseases and indirectly lead to deteriorating outcomes [5]. Pain is a constant feature of chronic conditions; failure or inability to manage and treat pain has been regarded globally as an abrogation of a fundamental human right [4] and considered a global public health problem [6]. In light of this, international organizations, such as the United Nations Economic and Social Council and the World Health Assembly, have also called on countries to ensure adequate availability of opioid analgesics and other pain medications [7,8]. Despite calls for the availability of pain medications to ensure the prompt and effective management of pain, an estimated 5 billion of the world’s population in 2009 had no or insufficient access to treatment of moderate to severe pain [9]. In 2014, the WHO estimated that, 80% of the global population had insufficient access to appropriate opioid analgesics for pain management [10]. Other studies globally have documented relatively low levels of usage of opioids analgesics and other pain medications for pain management in sub-Saharan Africa compared to other parts of the world particularly Europe [11,12]. In Africa for example, 91% of countries include opioids in their essential medicines list but only 13% have reported prompt availability of Morphine [13,14]. The limited availability of pain medications further burdens the already constrained healthcare system in the region as a result of inadequate pain management and treatment [3]. Reasons usually cited in the literature for the low levels of availability of pain medications include legal restrictions, deficiencies in the supply chain, lack of pharmacists in public health services, cultural misperceptions about pain, inadequate training of health-care providers, procurement difficulties, weak health systems and concerns about diversion, addiction and misuse [3-5,11,15-19].The African continent endures a high burden of pain and suffering from HIV/ AIDS and cancer but ironically receives and consumes the least amount of the world’s pain medications per capita particularly for opioids [3,5,20,21]. In 2008, there were 715 000 new cases and 542 000 cancer deaths in Africa, projected to reach 1.28 million new cases and 970 000 deaths by 2030 due to population growth and aging [22]. Likewise, as of the year 2018, the WHO African Region remained the most affected region by HIV/AIDS, with 25.7 million people living with HIV and 1.1 million new infections [23]. Thus, as the burden of HIV/AIDS and cancer continue to rise in Africa, the demand for pain medications will also rise. The management of pain and its associated suffering requires an effective health care delivery infrastructure, clinical skills and more importantly supplies that allow clinicians to prescribe and pharmacies to dispense drugs known to be most effective in the treatment of pain [24]. The need, therefore, arises for increased availability of pain medications including opioid analgesics in the healthcare system. However, information on the availability of pain medications in Ghana remains rudimentary. The few studies that report on availability of pain medicines in Africa principally focus on a narrow spectrum by type and distribution. This study seeks to scale up and provide comprehensive baseline information on the availability and distribution of pain medications across a broad spectrum of health facilities including public and private health facilities as well as community pharmacies and regional medical stores in Ghana. Indeed, the picture presently is not much different from that observed at the time of the survey.
Method
Study design
A cross sectional survey was conducted between April and June 2015 by reviewing records using a structured quantitative questionnaire from health facilities at all levels of care in all the then ten regions (presently 16 administrative regions) of Ghana.
Study population and sampling
The Study population involved all Ghana Health Service healthcare facilities at all levels of care as well as private hospitals, community pharmacies, the Christian Health Association of Ghana (CHAG) facilities, the Quasi Government Health Institutions (GAQHI) and the regional medical stores. The sample size was determined using a single population proportion estimation formula with 50% proportion, 10% of decision precision, 95% confidence interval and non-response rate of 20%. This resulted in a minimum sample of 121 health facilities. All regional hospitals were non-randomly sampled from the list of health institutions and same done for the regional medical stores. All the regional hospitals had a one-time review of their pharmacy for pain medication against a structured checklist (Appendix 1). The central medical stores had their records reviewed for pain medicines and findings recorded on the structured checklist for pharmacies. Two district hospitals, four health centres and eight community-based health planning and services (CHPS) compounds from each region were selected using simple random sampling as shown in Figure 1 below. Two Christian Health Association of Ghana (CHAG) facilities, private hospitals and private pharmacies were randomly selected from each region.
Data entry and statistical analysis
Research assistants were trained to capture the required information from designated focal persons using the structured interview guide. Data was captured by electronic mode. CSPro was used in programming the computer assisted personal interview (CAPI). The data was then exported to STATA (version 15) statistical package for data cleaning and analysis. Further accuracy and consistency checks among variables were done with STATA before the final analysis was made. Descriptive analysis of all recorded data was carried out to characterize the population studied. The main outcome of interest being the availability and distribution of pain medications were presented in frequencies with respective percentages.
Ethical statement
The study protocol was approved by the Ghana Health Service Ethics Review Committees with ID number: GHS ERC: 03/03/15. The protocol and questionnaires are available and annexed as supporting documents. The study was conducted in accordance with Good Clinical Practice.
Results
A total of 195 facilities were surveyed. Figure 2 shows information on the level and number of facilities surveyed. The facilities included maternity homes/community based health planning and services (CHPS) compounds; health centres; district, regional/teaching, specialist and
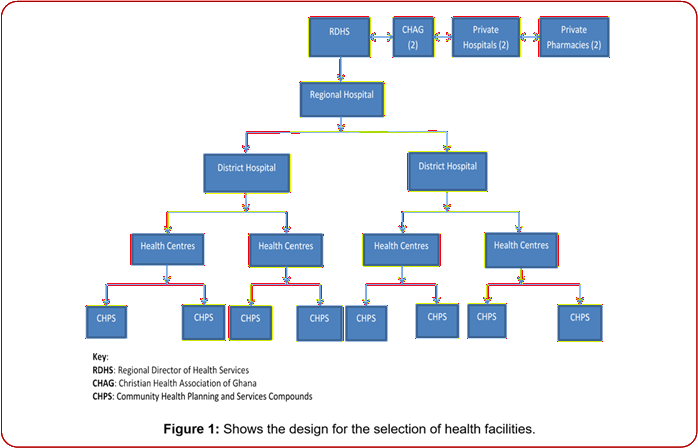
Figure 1: Shows the design for the selection of health facilities.
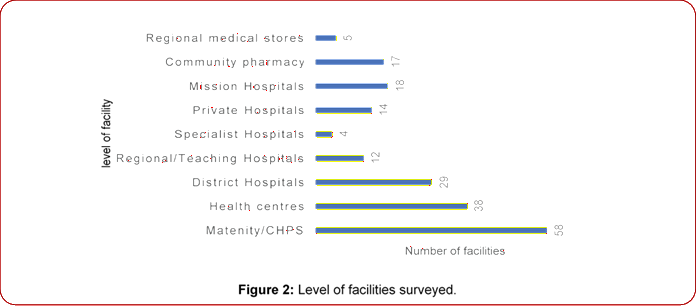
Figure 2: Level of facilities surveyed. private hospitals; community pharmacies and regional medical stores. The most reviewed facility type was CHPS compounds followed by health centres and the district hospitals.
Health facilities per regions
Table 1 presents information on the health facilities surveyed by location. With the exception of the Eastern region which had only 6 health facilities surveyed; all other regions had between 19 to 24 health facilities with the Northern region having the highest number of health facilities surveyed. Most of the health facilities were CHPS compounds (34.4%) followed by Health Centres (16.4%) and District hospitals (15.4%). No CHPS compound was surveyed in the Volta and Eastern regions and the Ashanti and Volta regions had no Health Centres surveyed.
Availability of analgesics and co-analgesics
Figure 3 shows the analgesics and co-analgesics that were available in the surveyed health facilities. Non-steroidal anti-inflammatory drugs (NSAIDs) were the commonest analgesic available in 168 out of the 195 facilities followed by opioids combined with other analgesics (101), selective Cox-2 inhibitors (30) with opioids analgesics available in 19 facilities. The commonest co-analgesic was benzodiazepines which was available in 145 facilities.
Opioids availability
The availability of opioid analgesic and opioid analgesic combinations in the various levels of health facilities surveyed is shown in Figure 4 below. Opioid analgesics were available in all the 4 specialist hospitals, 93% of surveyed district hospitals (27 out of 29), 83% of the regional/teaching hospitals (10 out of 12 facilities), 19% in Maternity/CHPS (11 out of 58) and 18% in the health centres (7 out of 38). Opioid analgesics in combination with other analgesics were much available in the community pharmacies (11 out of 17 surveyed). The higher-level surveyed facilities being the regional/teaching hospitals and the specialist hospitals had 1 and 2 facilities having these drugs respectively with none of the 5 surveyed regional medical stores having these opioid combinations.
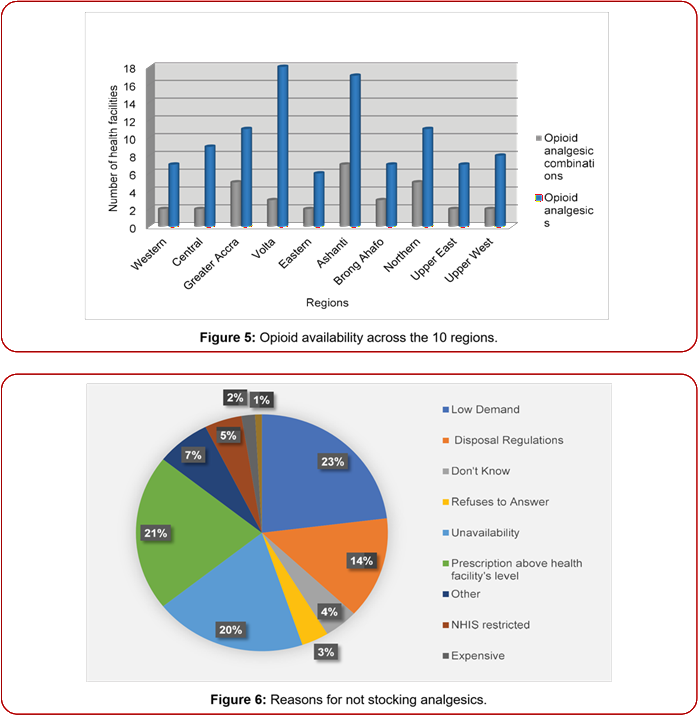
Opioid available across the regions
Volta region had the highest number of health facilities [18] that had opioid available followed by Ashanti region [17] with both Northern and Greater Accra regions having 11 each as shown in Figure 5 below. All the 6 surveyed health facilities in the Eastern region had opioids available but only 7 out of the 20 surveyed health facilities in the Brong Ahafo region having opioids. Availability of the opioid analgesic combinations was generally low with Ashanti region having them in 7 facilities and 5 facilities in both Northern and Greater Accra regions.
| Type of Health Facility, N (%) | ||||||||||
| Region | CHPS | Health | Regional/ | District | Specialist | Private | Mission | Community | Regional medical | TOTAL |
| Centre | Teaching | Hospital | Hospital | Hospital | Hospital | Pharmacy | Store | |||
| Hospital | ||||||||||
| Western* | 8(36.4) | 5(22.7) | 1(4.5) | 1(4.5) | 1(4.5) | 3(13.6) | 1(4.5) | 2(9.1) | 0(0) | 22(100) |
| Central | 8(38.1) | 5(23.8) | 1(4.8) | 2(9.5) | 0(0) | 0(0) | 2(9.5) | 3(14.3) | 0(0) | 21(100) |
| Greater | 8(42.1) | 4(21.1) | 1(5.3) | 3(15.8) | 1(5.3) | 0(0) | 1(5.3) | 0(0) | 1(5.3) | 19(100) |
| Accra | ||||||||||
| Volta | 0(0) | 0(0) | 1(5.3) | 8(42.1) | 1(5.3) | 4(21.1) | 3(15.8) | 1(5.3) | 1(5.3) | 19(100) |
| Region* | ||||||||||
| Eastern | 0(0) | 1(16.7) | 0(0) | 2(33.3) | 0(0) | 1(16.7) | 1(16.7) | 1(16.7) | 0(0) | 6(100) |
| Region | ||||||||||
| Ashanti | 9(42.9) | 0(0) | 1(4.8) | 5(23.8) | 0(0) | 1(4.8) | 1(4.8) | 3(14.3) | 1(4.8) | 21(100) |
| Brong- | 8(40) | 2(10) | 1(5) | 2(10) | 0(0) | 2(10) | 1(5) | 3(15) | 1(5) | 20(100) |
| Ahafo* | ||||||||||
| Northern* | 8(33.3) | 6(25) | 2(8.3) | 2(8.3) | 0(0) | 1(4.2) | 1(4.2) | 2(8.3) | 2(8.3) | 24(100) |
| Upper East | 9(42.9) | 5(23.8) | 1(4.8) | 1(4.8) | 0(0) | 2(9.5) | 0(0) | 2(9.5) | 1(4.8) | 21(100) |
| Upper West | 9(40.9) | 4(18.2) | 1(4.5) | 4(18.2) | 0(0) | 0(0) | 1(4.5) | 2(9.1) | 1(4.5) | 22(100) |
| TOTAL | 67(34.4) | 32(16.4) | 10(5.1) | 30(15.4) | 3(1.5) | 14(7.2) | 12(6.2) | 19(9.7) | 8(4.1) | 195(100) |
*These regions were split in 2018. Western North region created from Western region; Oti region from Volta region; Brong-Ahafo split into Ahafo, Bono and Bono East regions; and Northern region split into North East, Savannah and Northern regions
Table 1. Health facilities surveyed by region.
Reasons for not stocking analgesics
Reasons for not stocking these analgesics are depicted in the pie-chart below with 23% of surveyed facilities attributing it to low demand, 20% due to unavailability of these drugs, 21% saying most of these drugs were above their facility prescription level and 14% from disposal regulations. Interestingly, none was due to illicit use with only 5% attributing it with national health insurance scheme restrictions as shown in Figure 6. Some of the reasons given under others included the use of alternate analgesics preferably the NSAIDs and myths about the use of opioids.
Discussion
The main focus of this study was to investigate the availability of different classes of analgesic and co analgesic medications in public and private health facilities as well as community pharmacies and regional medical stores in Ghana. The study revealed that more than 70% of the 195 facilities surveyed had at least two of the 14 classes of these medications available. These were NSAIDs, which was in stock in 86.2% of the facilities and Benzodiazepines, a co-analgesic which was also available in 74.4% of the health facilities. All the remaining classes of surveyed medications were available in less than 35% of the health facilities reviewed with none of the facilities having Bupropion in stock. This finding confirms what is known in the literature about NSAIDs as the commonest and most widely used class of pain medications worldwide [25,26]. In a recent study in the United States of America (USA), 63% of the respondents reported usage of NSAIDs in the previous 12 months [27]. Approximately a quarter of health facilities prescribed opioids (27%) and opioids in combination with other pain medications (17%). These statistics portray a generally low level of availability of opioid medications in public and private health facilities in Ghana even in the present. Similar
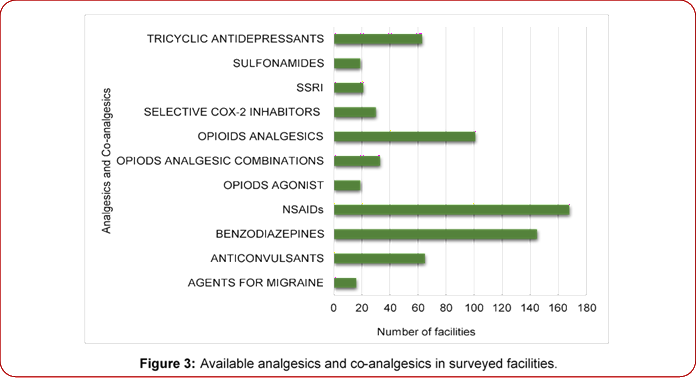
Figure 3: Available analgesics and co-analgesics in surveyed facilities.
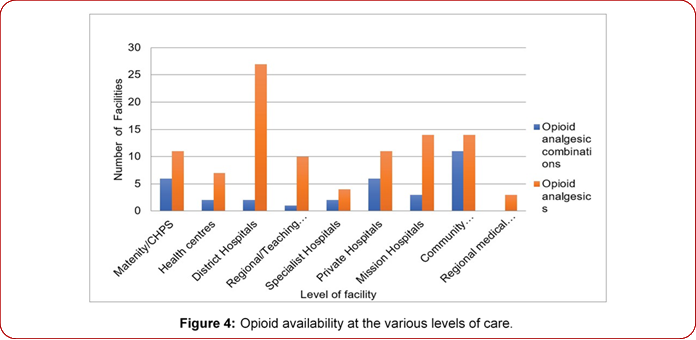
Figure 4: Opioid availability at the various levels of care.
studies have found relatively low levels of availability and consumption of opioid analgesics in Africa, Asia, Central America, the Caribbean, South America compared to European countries [11,20,28-30]. A study of 120 health facilities in Kenya and Uganda showed only 7% of facilities had access to morphine [12]. Another study by Cleary et al in 25 African countries found Codeine and Morphine as the primary and most common opioid formularies available in the countries surveyed and only 3 countries, Algeria, Mauritius and Morocco had 6 of the 7 opioids available [20].
The availability of pain medications as revealed by this study, varied across the different facilities surveyed. Among all the facilities surveyed community pharmacies were the most stocked with pain medications followed by
the hospitals, regional medical stores, health centres and CHPS compounds in that order. The situation at the CHPS compounds and Health centres was profound with as many as seven classes of pain medications not available in any CHPS compound and five classes of pain medications not available in any health centre. The healthcare system of Ghana has five levels of providers: CHPS compounds, health centres, district hospitals, regional hospitals and tertiary hospitals [31]. Thus, the lowest levels of healthcare provision in Ghana which is at the heart of and also the foundation of primary health care recorded the lowest availability of pain medications. This, however, is coherent with the volume of clients as well as the range of services provided compared to the higher levels of health care delivery such as the regional and district hospitals. Despite this fact, since pain is the most common reason for medical consultations generally, it’s appropriate for all levels of healthcare provision to be equally stocked with different classes of pain medications irrespective of their average client volumes or level of care. Similar findings have been revealed in a study of 120 health facilities in East-Africa which also detected varying levels of availability of pain medications among different levels of healthcare facilities with the lower levels of care usually having lower stock levels [12].
The reasons given in most facilities for the unavailability of some class of pain medications were low demand for pain medications, unavailability of these medications, above health facility prescription level and disposal regulations governing medicine stocks. These findings are consistent with evidence in the pain medication literature that highlight factors known to have exacerbated the low stock levels of pain medications in healthcare systems globally [32-34]. Some of these factors include the cost of pain medicines [35], excessively restrictive drug control regulations or enforcement practices which sometimes stem from misconceptions and fears about opioids, so-called opiophobia [20,36-42], failure to enact palliative care and pain treatment policies, failure to ensure the functioning and effective supply system among others [5,41] as well as poor prescriber knowledge of pain and the principles of management [43-46] and NSAID misuse [27].
The study has also highlighted the need for efficient strategies to ensure prompt and constant availability of all classes of pain medications at all levels of the healthcare delivery system in line with the national essential medicine guidelines. In other jurisdictions, campaigns to promote pain medications availability have been taken up by human rights organizations and the results have been encouraging [47]. Moreover, with the global emergence and re-emergence of diseases and infections such as SARS CoV-2 which is clinically managed in part with opioids such as morphine, fentanyl and midazolam because of its prevalent respiratory symptoms of breathing difficulty and cough [34], the need for the availability and access to all varieties of pain medications is even more compelling. The whole healthcare system in Ghana, therefore, needs strategic restructuring that can ensure prompt availability of pain medications for the effective management of pain related morbidities to relieve preventable suffering.
Conclusion
The high usage of NSAIDS is worrying if no proper education and supervision is ensured because of its potential side effects. Similarly, the ready availability of benzodiazepines should prompt responsible authorities including the Ghana Food and Drug Authority to increase regulatory activities to stem its potential abuse. Meanwhile, the ready availability of opioids in District hospitals than Regional and Teaching hospitals reflects an anomaly that requires further investigation and same applies to the availability of opioid analgesic combinations in community pharmacies which are less likely to be as regulated as the hospitals. “Low demand”, the prevalent reason afforded for not stocking analgesics especially opioids highlight issues with knowledge and competencies in pain management that needs urgent attention. In light of these findings, further studies are needed to quantify the actual consumption of pain medications and their co-analgesics so as to make available the right quantities to the various regions and facilities to prevent excesses that may expire or get diverted and avoid shortages that may compromise optimal pain management. Understanding the reasons for this distribution is quite essential and was concurrently captured in a qualitative study, findings of which will be made public in a subsequent paper. The broader picture of essential medicines used in palliative care and pain management was similarly captured and will as well be made available.
Acknowledgement
None
Source of funding
None
Conflict of interest
None to report
References
1. Van den Beuken-van Everdingen MHJ, JM De Rijke, AG Kessels and HC Schouten, et al. “Prevalence of Pain in Patients with Cancer: ASystematic Review of the Past 40 Years.” Ann Oncol 18(9) (2007): 1437-
1449.
2. Schappert, Susan M. National Ambulatory Medical Care Survey: 1990 summary. No. 203. US Government Printing Office, 1992.
3. NchakoElmang, Scottie Bussell, Carlos Nesbeth and ChisomOdoh. “Barriers to the Availability and Accessibility of Controlled Medicines for Chronic Pain in Africa.” Int Health 10 (2018): 71-77.
4. Brennan Frank, Daniel B Carr and Michael Cousins. “Pain Management: AFundamental Human Right.” AnesthAnalg 105 (2007): 205-221.
5. LohmanDiederik, Rebecca Schleifer and Joseph J Amon. “Access to Pain Treatment as a Human Right.” BMC Med 8 (2010): 1-9.
6. Gilson Aaron M, Martha A Maurer, Virginia T LeBaron and Karen MRyan, et al. “Multivariate Analysis of Countries Government and Health-care System Influences on Opioid Availability for Cancer Pain Relief and Palliative Care: More than a Function of Human Development.” Palliat Med 27 (2013): 105-114.
7. United Nations. Treatment of Pain Using Opioid Analgesics.
8. World Health Organization. Cancer Prevention and Control, World Health Assembly (Resolution 58.22). 2005; Available from: www.who.int/cancer/media/ news/WHA58 22-en.pdf
9. World Health Organization. World Health Organization Briefing Note — February 2009:Access to Controlled Medications Programme. Geneva; 2009.
10. Connor, Stephen R and Maria Cecilia Sepulveda Bermedo. “Global Atlas of Palliative Care at the End of Life.” (2018).
11. Berterame Stefano, Juliana Erthal, Johny Thomas and Sarah Fellner, et al. “Use of and Barriers to Access to Opioid Analgesics: A Worldwide, Regional, and National Study.” Lancet 387 (2016): 1644-1656.
12. Harding Richard, Victoria Simms, Suzanne Penfold and Julia Downing, et al. “Availability of Essential Drugs for Managing HIV-related Pain and Symptoms within 120 PEPFAR-funded Health Facilities in East Africa: A Cross-sectional Survey with Onsite Verification.” Palliat Med 28 (2014): 293-301.
13. ChernyNI, JCleary, W Scholten and L Radbruch, et al. “The Global Opioid Policy Initiative (GOPI) Project to Evaluate the Availability and Accessibility of Opioids for the Management of Cancer Pain in Africa, Asia, Latin America and the Caribbean, and the Middle East: Introduction and methodology.” Annals Oncol 24 (2013): xi7-xi13.
14. Cherny NI, J Baselga, FDConno and L Radbruch. “Formulary Availability and Regulatory Barriers to Accessibility of Opioids for Cancer Pain in Europe: AReport from the ESMO/EAPC Opioid Policy Initiative.” Annals Oncol 21 (2010): 615-626.
15. O’Brien Megan, Faith Mwangi-Powell, Isaac FAdewoleandOlaitanSoyannwo, et al. “Improving Access to Analgesic Drugs for Patients with Cancer in Sub-Saharan Africa.” Lancet Oncol14(2013): e176-e182.
16. Mwangi-Powell, Faith. “Palliative Care and Public Health, APerspective from the African Palliative Care Association.” J Public Health Policy 28 (2007): 59-61.
17. Linge-DahlLisa, MarjoleinVranken, SaskiaJuenger and Kate North, et al. “Identification of Challenges to the Availability and Accessibility of Opioids in Twelve European countries: Conclusions from two ATOME Six-Country Workshops.” J Palliat Med 18(2015): 1033-1039.
18. Clark Joseph, Sam Gnanapragasam, Sarah Greenley and Jessica Pearce, et al. “Perceptions and Experiences of Laws and Regulations Governing Access to Opioids in South, Southeast, East and Central Asia: A Systematic Review, Critical Interpretative Synthesis and Development of a Conceptual Framework.” Palliat Med 35(2021): 59-75.
19. ClarkJoseph, NaveenSalins, Sunitha Daniel, and David CCurrow,et al. “Views and Experiences of Opioid Access Amongst Palliative Care Providers and Public Representatives in a Low-Resource Setting: A Qualitative Interview Study.” PLOS Global Public Health 3 (2023): e0002401.
20. Cleary, JamesLRadbruch, J Torode and NI Cherny. “Formulary Availability and Regulatory Barriers to Accessibility of Opioids for Cancer Pain in Asia: AReport from the Global Opioid Policy Initiative (GOPI).” Annals Oncol 24 (2013): xi24-xi32.
21. Powell RichardA,Richard Mugula Kaye, Henry Ddungu and Faith Mwangi-Powell. “Advancing Drug Availability—Experiences from Africa.” J Pain Symptom Manag 40(2010): 9-12.
22. Ferlay Jacques, Hai‐Rim Shin, Freddie Bray and David Forman, et al. “Estimates of Worldwide Burden of Cancer in 2008: GLOBOCAN 2008.” Int J Cancer 127 (2010): 2893-2917.
23. World Health Organization (WHO). HIV/AIDS. 2019.
24. NakanjakoDamalie, Robert Colebunders, Alex GCoutinhoandKamya. “Strategies to Optimize HIV Treatment Outcomes in Resource-Limited Settings.” AIDS Rev 11 (2009): 179-189.
25. Cleveland Clinic. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs). Cleveland Clinic 2021.
26. Griffin M. Pain Relief: How NSAIDs Work. WebMD. 2005.
27. CryerByron, Michael A Barnett, Jennifer Wagner and C Mel Wilcox. “Overuse and Misperceptions of Nonsteroidal Anti-Inflammatory Drugs in the United States.” Am J Med Sci 352(2016): 472-480.
28. Ponizovsky Alexander M, Michael VPChelintsev and Eli Marom, et al. “Differences in the Consumption Rates and Regulatory Barriers to the Accessibility of Strong Opioid Analgesics in Israel and St. Petersburg.” Eur J ClinPharmacol 68 (2012): 89-95.
29. Manjiani Deepak, D Baby Paul, Sreekumar Kunnumpurath and Alan David Kaye, et al. “Availability
and Utilization of Opioids for Pain Management: Global Issues.” Ochsner J14 (2014): 208-215.
30. Seya Marie-Josephine, Susanne FAM Gelders, ObianujuUzomaAchara and Barbara Milani, et al. “A First Comparison between the Consumption of and the Need for Opioid Analgesics at Country, Regional, and Global levels.” J Pain Palliat Care Pharmacother 25(2011): 6-18.
31. Pharmaccess Foundation. A CLOSER LOOK AT THE HEALTHCARE SYSTEM IN GHANA. 2016.
32. Namisango Eve, Matthew J Allsop, Richard A Powell and Stefan J Friedrichs Dorf, et al. “Investigation of the Practices, Legislation, Supply Chain, and Regulation of Opioids for Clinical Pain Management in Southern Africa: AMulti-Sectoral, Cross-National, Mixed Methods Study.” J Pain Symptom Manag55(2018): 851-863.
33. Ooms, Gaby Isabelle, Paul KlatserandHendrika A, et al. “Barriers to Accessing Internationally Controlled Essential Medicines in Uganda: AQualitative Study.” J Pain Symptom Manag 58(2019): 835-843.
34. Pettus Katherine, James F Cleary, Liliana de Lima and Ebtesam Ahmed, et al. “Availability of Internationally Controlled Essential Medicines in the COVID-19 Pandemic.” J Pain Symptom Manag 60(2020): e48-e51.
35. De Lima Liliana, Natalia Arias Casais, Roberto Wenk andLukas Radbruch, et al. “Opioid Medications in Expensive Formulations are Sold at a Lower Price than Immediate-Release Morphine in Countries throughout the World: Third Phase of Opioid Price Watch Cross
Sectional Study.” J Palliat Med 21 (2018): 1458-1465.
36. Mpogoro Filbert J, DismasMatovelo, AliyahDosani and SospatroNgallaba, et al. “Uptake of Intermittent Preventive Treatment with Sulphadoxine Pyrimethamine for Malaria during Pregnancy and Pregnancy Outcomes: ACross-Sectional Study in GeitaDistrict, North-Western Tanzania.” Malaria J 13 (2014): 1-14.
37. Krakauer Eric L, Nguyen Thi Phuong Cham, SyedaAsra Husain and Nguyen ThiHai Yen, et al. “Toward Safe Accessibility of Opioid Pain Medicines in Vietnam and Other Developing Countries: ABalanced Policy Method.” J Pain Symptom Manag 49(2015): 916-922.
38. Scholten Willem. “Improving Access to Adequate Pain Management in Taiwan.” ActaAnaesthesiologicaTaiwanica 53(2015): 62-65.
39. VrankenMarjolein JM, Lisa Linge-Dahl, Aukje K Mantel-Teeuwisse and Lukas Radbruch, et al. “The Perception of Barriers Concerning Opioid Medicines: A Survey Examining Differences Between Policy Makers, Healthcare Professionals and Other Stakeholders.” Palliat Med 34 (2020): 493-503.
40. VrankenMarjolein JM, Aukje K Mantel-Teeuwisse, SaskiaJungerandLukas Radbruch, et al. “Legal Barriers in Accessing Opioid Medicines: Results of the ATOME Quick Scan of National Legislation of Eastern European Countries.” J Pain Symptom Manag48(2014): 1135-1144.
41. Xhixha, Ali, RudinaRamaand Lukas Radbruch. “Reducing the Barriers to Pain Management in Albania: Results from An Educational Seminar with Family Doctors.” J Palliat Med 16 (2013): 758-761.
42. Yao Jane S, Odette D Kibu, Constantine Asahngwa and Ngo V Ngo, et al. “A Scoping Review on the Availability and Utilization of Essential Opioid Analgesics in Sub-Saharan Africa.” Am J Surg (2023).
43. Lohman, Diederik, Rebecca Schleifer and Joseph JAmon. “Access to Pain Treatment as a Human Right.” BMC Med 8 (2010): 1-9.
44. Joranson, David E. “Availability of Opioids for Cancer Pain: Recent Trends, Assessment of System Barriers, New World Health Organization Guidelines, and the Risk of Diversion.” J Pain Symptom Manag 8(1993): 353-360.
45. AlotaibiKhalaf, I Higgins, J Dayand SChan. “Paediatric Pain Management: Knowledge, Attitudes, Barriers and Facilitators Among Nurses–Integrative Review.” IntNurs Rev 65 (2018): 524-533.
46. AregayAtsede, Margaret O’Connor, Jill Stow and Nicola Ayers, et al. “Perceptions of Barriers to Using Opioid Analgesics: AMixed Methods Study.” Palliat Med Rep 4(2023): 249-256.
47. Lohman, Diederik and Joseph J Amon. “Evaluating AHuman Rights-Based Advocacy Approach to Expanding Access to Pain Medicines and Palliative Care: Global Advocacy and Case Studies from India, Kenya, and Ukraine.” Health & Hum Rts J17 (2015): 149.