Soheil Salari3*, Yasaman Bozorgnia1, Mina Moradi2, Zahra Sadeghi4
1Department of Orthodontics, North Khorasan University of Medical Sciences, Bojnurd, Iran
2Department of Orthodontics, North Khorasan University of Medical Sciences, Bojnurd, Iran
3Department of Orthodontics, Aja University of Medical Sciences, Tehran, Iran
4Student Research Committee, Department of Orthodontics, North Khorasan University of Medical Sciences, Bojnurd, Iran
*Correspondence: Soheil Salari, Department of Orthodontics, Aja University of Medical Sciences, Tehran, Iran, Email: soheilsalari@gmail.com
Received: 19 Nov, 2025; Accepted: 13 Dec, 2025; Published: 24 Dec, 2025.
Citation: Soheil Salari, Yasaman Bozorgnia, Mina Moradi, Zahra Sadeghi. “Bracket failure rates using single vs. two-component orthodontic adhesives: A 6-month split-mouth clinical trial.” J Oral Dis Treat (2025):110. DOI: 10.59462/JODT.2.1.110
Copyright: © 2025 Soheil Salari. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribu tion, and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: A good bonding is a crucial stage in orthodontic treatments. In this six-month clinical trial, our aim was to compare clinical bonding failure of a single component orthodontic adhesive with a standard two-component adhesive which needs primer separately.
Materials and Methods: This study was a randomized split-mouth prospective clinical trial. 50 patients (50 upper jaws and 50 lower jaws) were selected from a private clinic. They all underwent comprehensive orthodontic treatment using 0.022-inch slot appliances. Randomly, one side was bonded with a single component orthodontic adhesive [GC Ortho Connect (GC)], that did not require primers; and the opposite side was bonded with a standard twocomponent adhesive [Transbond XT]; which required a primer. For each patient, failure rate of brackets was recorded after 6 months.
Results: There was no significant difference between bonding failure rate of Transbond XT (1.19%) and GC Ortho Connect (0.91%) (P-value= 0.67%). There was also no significant difference between bonding failure in maxilla and mandible (P = 0.67) and between the genders (P =0.2); but bonding failure in posterior teeth were significantly higher than anteriors. (p<0.0001)
Conclusions: Our study showed that clinical bonding failure of the single-component orthodontic adhesive (GC Ortho Connect) was less than the control group, although not significant. Because of the lack of the primer stage, the clinician can have a better saliva contamination and moisture control. Moreover, the chair time would be less.
Clinical Relevance: The study is a complete clinical trial and the results of our study may help the clinicians, and also the patients, a lot by reducing the chair time.
Introduction
Everyday new materials and techniques are introduced to improve orthodontic bracket bonding; for instance, new adhesives, self-etching primers, bracket materials, bracket base designs or different curing methods to cure more efficiently and faster [1].
In conventional bonding method, the enamel is cleaned and conditioned, primer then applied on tooth surface, light cured and then the adhesive is applied on the base of the bracket. After that the bracket is positioned on the tooth and cured for ten seconds from each side of the bracket. The more time needed for this bonding procedure and the more risk of moisture contamination may we have, could result into clinical bonding failure. [2] For this reason, Self Etch Primer (SEP) was introduced to the market that combined etching and priming the enamel at once.
In literature, there were no significant differences among this method and the conventional one after a 6-month period.[3] Another approach also appeared that combined the primer with the adhesive to reduce the working time. [4]Bearing in mind that we cannot precisely create a natural oral environment in vitro, clinical bond failure studies were used to examine the survival of proper bracket bonding. [5]
Many studies were done to evaluate the bonding failure rates of different types of adhesives, but thy were mostly done on two-stage conventional bonding systems (etching + Transbond XT adhesive primer) and single-stage Self-Etching Primer (SEP)(TransbondPlus). [6-13]
There are few studies about efficacy of single component orthodontic adhesives that did not require primers compared to the standard two-component adhesives. An in vitro study compared microleakage and shear bond strength of them on metal and ceramic brackets and reported that they can be used safely instead of each other. [14] In another study they compared survival rate of indirectly bonded brackets with use of single vs. two-component orthodontic adhesives. They concluded there is a tendency for debonding in the single component group but that was not statistically significant. [15]
The purpose of the present study was to perform a 6-month clinical assessment of the failure rates of brackets directly bonded with GC Connect Ortho (adhesive integrated into the primer) and Transbond XT (Conventional Adhesive). The number of bracket failure was also compared between dental arches, regions and genders.
Methods and Materials
This study was approved by the Ethical Committee of North Khorasan University of Bojnurd, Iran. This single blind clinical trial was done on 50 patients needing comprehensive orthodontic treatment in both jaws. The whole process was performed by a single orthodontist in a private clinic in Bojnurd, Iran. The study included patients with permanent teeth fully erupted, from central incisors to first molars, with no decalcification or restoration on buccal surfaces of the teeth. The patients all had good oral hygiene. The
ones who needed orthosurgery were excluded.For bonding the brackets, a same protocol was applied. First oral prophylaxis was done for 10 seconds with pumice. Then the tooth was rinsed for 10 seconds with water. Enamel was etched with 37% phosphoric acid for 30 seconds, followed by rinsing and drying for 5-10 seconds.
We had two adhesive systems for the control and treatment groups: Treatment group (one-step orthodontic adhesive); 37% phosphoric acid + GC Ortho Connect light cure adhesive (GC Orthodontics, Breckerfeld, Germany). Control group (two-step totaletch adhesive): 37% phosphoric acid + Transbond XT primer + Transbond XT light cure adhesive (3M Unitek, Monrovia, Calif). A split-arch technique was used, in which one quadrant of maxillary arch and the other quadrant of mandibular arch were bonded with the treatment group adhesive and the other sides were bonded with the control group adhesive. The sides were randomly selected by coin toss.The brackets were then placed on the teeth and pressed with a constant force. Then the surrounding flash of the adhesive was carefully removed by a sickle scaler and light cured by LED for 40 seconds (10 seconds for each side of brackets). After bonding the entire quadrant, each patient was educated how to deal with the brackets and maintain the oral health. Every month the patient was visited and if any bracket was debonded it was recorded and the tooth was no longer followed in the study.
To make it a blind study, after 6 months, another operator collected the data from the patients’ records about the debonded brackets and the date of the debonding. After all the brackets were recorded, then it was revealed which bracket was bonded with whcih adhesive system (A or B). This was only known for the first operator.
The significant differences in the bracket survival rate among the two adhesives, patient gender, location in the maxilla or mandible and position of the tooth in anterior or posterior region were determined with the Kaplan-Meier product limit survival estimates and the log-rank test at P <0.05.
Results
50 patients participated in this study. Total of 1095 teeth were bonded (548 with Transbond XT and 547 with GC Ortho Connect). During the six- month follow-up, the mean survival time for brackets bonded with Transbond XT and GC Ortho Connect was 177.35 and 178.04 days respectively. It showed no statistically significant difference. In this 6-month period, a total of 23 bracket bonds failed (bond failure rate of 2.1%). Bonding failure rate with GC Ortho Connect and Transbond XT was 0.91 % and 1.19%, respectively. However, the Kaplan- Meier survival distribution test showed no statistically significant correlation between the type of bonding material and bracket failure rates (P=0.52). (Figure 1)
Bonding failure rate in posterior segment was 2.01% (mean survival time =175.39 days). In anterior segment it was 0.09% (mean survival time =179.84 day), which showed a statistically significant difference (p<0.0001) (Figure 2).
The maxillary brackets had a failure rate of 1% (survival time range between 175.77-178.97 days) whilst the mandibular ones had a 1.1% failure rate (survival time range between 176.67-179.42 day). There was no statistically significant difference between the arches (P=0.77) (Figure 3). Mean survival time for the boys were 177.14 days and for the girls it was 177.87 days. There was no statistically significant difference between the genders too. (p=0.18) (Figure 4)
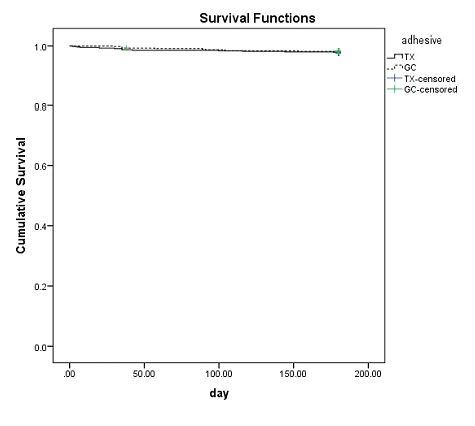
Figure 1: Overall Kaplan-Meier survival plot comparing bond failure between Transbond XT and GC Ortho Connect
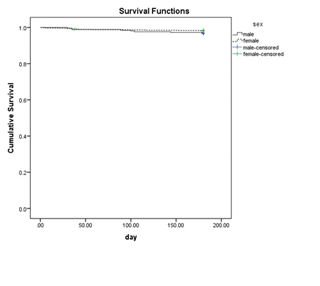
Figure 2: Overall Kaplan-Meier survival plot comparing bond failure in anterior and posterior segments.
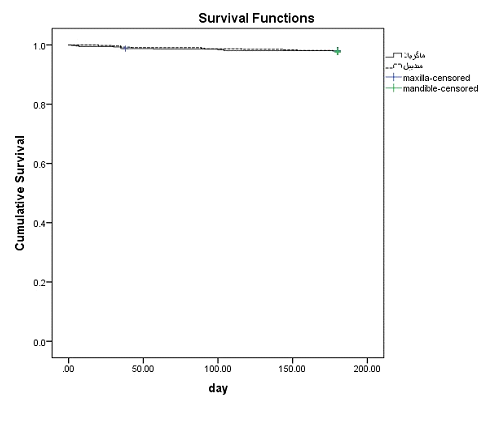
Figure 3: Overall Kaplan-Meier survival plot comparing bond failure in maxillary and mandibular arches
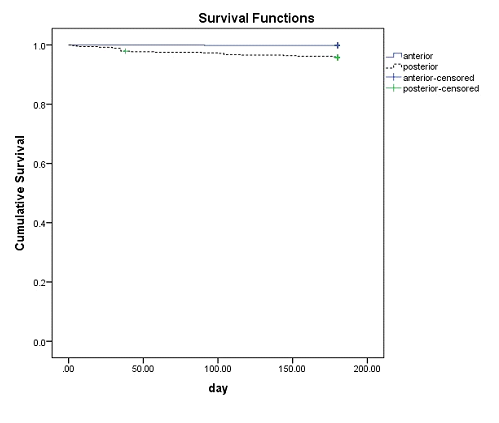
Figure 4: Overall Kaplan-Meier survival plot comparing bond failure in boys and girls
Discussion
Orthodontic attachments bonded to enamel surface are applied for a certain time. The bond strengths of adhesives should be high enough to hold the bracket on the tooth surface, but also low enough to cause no damage to the enamel surface during debonding procedure and allow easy cleaning of the remnants.[16]
The working time for one-step adhesives would be less, with less risk of contamination with saliva or blood. We tried to compare bonding failure rate of this system with the traditional two-step adhesives to figure out if they can be replaced each other or not.
We found 13 bracket bond failure in a 6-month period for Transbond XT (1.9%) and 10 bracket bond failure for GC Connect Ortho (0.9%), which showed no statistically significant differences between them (p=0.52). In the same period, failure rates of 8.1% and 3.6% for Transbond XT, respectively [17,18]. [19]reported a boning failure of 1.7% in a period of 12 months, while [8] reported a 4.4% rate in 24 months for Transbond XT. The results of the studies are different and it is probably due to the lack of a standardized protocol, different patients and different operators. [19] Bonding failure rate of less than 10% is considered clinically accepted. [20]
Many articles compared failure rate of different bonding systems with Transbond XT as a gold standard. [17] used Heliosit Orthodontic (6% bond failure), [18]. used Orthofix (2.7% bond failure), [19]. compared Green Gloo (5% bond failure) and [8]. compared Transbond plus (4.7% bond failure). In all of the above-mentioned articles, there were no significant differences found between these adhesives and Transbond XT. [8, 17-19]
In our study, no significant differences were found between failure rate in maxilla and mandible. Bonding failure rate in maxilla was 1% (mean survival time = 177.37 days) while in mandible it was 1.1% (mean survival time = 178.04 days); similar results were found in some articles. [8, 17, 20-24]
While some articles reported more bracket failure in mandible, this can be related to more masticatory load on the mandibular brackets, more potential for mandibular brackets to have an interference and/or contact in centric relation and more saliva contamination in posterior region of the mandible during the bonding procedure. [22, 25-28]
We found out that bond failure in posterior region was higher than the anterior (bond failure rate in posterior teeth was 2.01% and mean survival time was 175.39 days; while in anterior teeth bond failure rate was 0.09%, and mean survival time was 179.84 days). Bond failure may differ in different sites of the mouth. This can be caused by higher mastication forces in posterior region (30 kg in posterior in comparison to 13-15 kg in anterior region), difficulty to access and manipulate the posterior region for bracket placement, difficulty in moisture control, inadequate bonding surface because of tooth morphology and different enamel structure (for example, more aprismatic enamel on premolars). [29,30]Our results are in consistent with previous studies which showed the bond failure rate is higher in posterior teeth than anteriors, [17]. reported more bonding failure in anterior teeth; although not significant. [8, 12, 17, 21, 23, 26, 31]
Even with the use of a standard protocol, same adhesive and same operator, bonding failure rate is different for different teeth and sites. Some parts of the mouth could be more susceptible to bond failure due to tooth morphology, masticatory forces and chewing patterns. [17]
Patient gender did not influence failure rates. This is in accordance with the clinical studies conducted by [8, 20, 22, 24]. [32], reported almost twice failure in male patients compared with female patients in a 5-year survey. This can be due to more cautiousness and more motivation of females for esthetic treatments. Also we should bear in mind that in his study different operators with different mechanics and different bracket systems were used. [32]
We used the split-mouth technique to reduce inter individual variability. A unique operator used the standard bonding protocols for two bonding systems in a same day. Therefore, difference in nutrition or oral habits were eliminated. Moreover, it was observed that the post-gel polymerization values of this one-step orthodontic adhesive were significantly higher compared to Transbond (3M Unitek). [33], GC Ortho Connect can be used safely instead of the two step total-etch adhesives due to less microleakage and adequate SBS values for bonding of metal and ceramic brackets. [14]This study suggests that both GC Ortho Connect and Transbond XT can be used for bonding the brackets securely.
CONCLUSIONS
Our randomized controlled trial showed that failure rates of bonding brackets with GC Ortho Connect is less (but not statistically significant) than the conventional adhesive (Transbond XT); therefore, clinically approved and acceptable.GC Ortho Connect can be advantageous in terms of eliminating the need for primers, facilitating the bonding procedure, saving chair time and reducing the potential errors related to contamination with saliva. Moreover because of the less viscosity, it can be applied to the mesh base of the brackets easier.
Conflict of Interests
The authors want to declare that they did not have any financial or non-financial conflict of interests.
Ethics Approval
This study was approved by the Ethical Committee of North Khorasan University of Bojnurd, Iran
Funding
Not applicable
References