Sheeba S1*, Ramya S. S2, Sanju S3, Reshma Reghu4 and Gokul Krishna5
1Department of Gynaecology and Obstetrics, Sarada Krishna Homoeopathic Medical College. (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Tamilnadu, India
2Department of Homoeopathic Pharmacy, Sarada Krishna Homoeopathic Medical College, (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Tamilnadu, India
3Department of Forensic Medicine, Sarada Krishna Homoeopathic Medical College, (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Tamilnadu, India
4Department of Community Medicine, Sarada Krishna Homoeopathic Medical College, (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Tamilnadu, India
5Department of Material Medical, Sarada Krishna Homoeopathic Medical College, (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Tamilnadu, India
*Correspondence: S Sheeba, Department of Obstetrics and Gynaecology, Sarada Krishna Homoeopathic Medical College, (Affiliated to The Tamil Nadu Dr. M.G.R. Medical University, Chennai), Kulasekharam, Kanyakumari District, Tamilnadu, India. E-mail: sheeba.syduu@gmail.com
Citation: Sheeba S, Ramya SS, & Sanju S et al. “Clinical Efficacy of Anti-Miasmatic Treatment in the Management of Polycystic Ovarian Disease: Reflections on Homeopathic Perspective.” J Gynecol Matern Health (2026): 129. DOI: 10.59462/3068-3696.4.1.129
Received date: 28 Jan, 2026; Accepted date: 11 Feb, 2026; Published date: 18 Feb, 2026
Copyright: © 2026 Sheeba S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Polycystic Ovarian Disease (PCOD) is a hormonal disorder in women, characterized by enlarged ovaries and the presence of multiple small cysts along the outer edge of the ovaries. It is a multifactorial and polygenic condition, primarily resulting from an imbalance in reproductive hormones, particularly the excessive production of androgens. This hormonal disturbance leads to typical ovarian changes such as inflammation, increased ovarian volume, a thickened capsule, and a distinctive pearly white appearance. The most common clinical manifestations of PCOD include obesity, menstrual irregularities such as oligo-ovulation, anovulation, Oligomenorrhoea, amenorrhea, infertility, dysfunctional uterine bleeding, hirsutism, acne, HAIR-AN syndrome, and features of Hyperandrogenism. In this study, ten clinically diagnosed PCOD cases were selected and analysed. The objective was to explore the therapeutic potential of individualized homeopathic treatment based on the principle of similimum. Medicines such as Thuja Occidentalis, Natrum Muriaticum, Calcarea carbonica, and Oophorinium were prescribed according to symptom similarity and holistic assessment. A gradual improvement in clinical symptoms was observed in all cases. Moreover, these remedies played a significant role in managing associated complaints and reducing the recurrence of symptoms an area where conventional medicine often faces challenges.
Keywords: Androgen, Anovulation, Hirsutism, Polycystic Ovarian Disease, Polygenic disorder.
Polycystic Ovarian Syndrome (PCOS) was first described in 1935 by Stein and Leventhal, who observed a clinical pattern characterized by amenorrhea, hirsutism, obesity, and enlarged polycystic ovaries [1]. It is a heterogeneous endocrine disorder primarily marked by excessive androgen production by the ovaries. PCOS is a multifactorial and polygenic condition, with a prevalence rate ranging between 30–40% among women of reproductive age. Interestingly, polycystic ovarian morphology may be observed in approximately 55% of otherwise healthy women [2]. PCOS is recognized as the most common endocrine disorder affecting women between the ages of 18 and 39. The etiological factors include follicular cysts, corpus luteal cysts, and theca-lutein cysts [3], which are often associated with hormonal imbalances. These imbalances result in clinical features such as irregular menstruation or amenorrhea, anovulation, heavy menstrual bleeding, hirsutism, acne, pelvic discomfort, infertility, and patches of thickened, darkened skin (commonly on the neck and face).
The syndrome is also strongly associated with insulin resistance and obesity [4], which contribute to weight gain and can predispose individuals to metabolic syndrome and type 2 diabetes [5]. Genetic predisposition plays a significant role in PCOS, as many patients report a family history of the condition [6]. The early phase of the menstrual cycle, referred to as the follicular phase, is characterized by a rise in follicle-stimulating hormone (FSH), which stimulates the development of a dominant follicle, preparing it for ovulation [7]. However, in PCOS, ovulation may not occur due to excess androgens that disrupt this process, leading to symptoms such as hirsutism and acne [8]. Because the symptoms are often nonspecific or overlooked, PCOS can be challenging to diagnose in its early stages.
During the follicular phase, the failure of normal follicular development and the absence of a luteinizing hormone (LH) surge can prevent ovulation [9]. The resulting follicular cysts typically range from 2.5 mm to 9 mm in diameter and may manifest as abnormal hair growth [10]. The granulosa cells surrounding these cysts can persist, producing excess estradiol, which contributes to irregular menstruation or menorrhagia [11]. Women with PCOS commonly experience irregular or missed periods due to anovulation [12]. Furthermore, the HAIR-AN syndrome—characterized by Hyperandrogenism, insulin resistance, and acanthosis nigricans—is often observed in patients with PCOS [13].
Materials and Methods
A sample of ten cases of Polycystic Ovarian Disease (PCOD) was selected using a random sampling technique from the outpatient department, inpatient ward, and peripheral units of our hospital. These cases were evaluated to investigate the prevalence and characteristics of PCOD. The study population included women aged between 14 and 35 years, who were further categorized for detailed analysis. Each case underwent a comprehensive assessment involving a thorough clinical history, physical examination, and ultrasonography evaluation. The objective of this study was to identify the common causative factors and menstrual irregularities associated with PCOD, and to evaluate the efficacy of individualized Homoeopathic treatment in its management. A comparative analysis of each case was conducted before and after Homoeopathic intervention, with patients observed for a minimum duration of 3 to 6 months.
Case-taking was systematically conducted using the SKHMC format. A total of 10 cases were included in the study based on the presence of characteristic symptoms. Clinical features such as obesity, menstrual irregularities (Oligomenorrhoea, amenorrhoea, or dysfunctional uterine bleeding), infertility, hirsutism, acne, and signs of insulin resistance such as thickened pigmented skin or acanthosis nigricans were noted and analysed through Repertorization. [14,15]. Prescriptions were made in accordance with the principles of Homoeopathy, following the guidelines laid out in the Organon of Medicine and standard texts of Materia Medica. Repetition of doses was determined based on individual response to treatment. Improvements were primarily assessed through symptomatic relief, and findings are documented in Table 1 and Table 2. Statistical methods were employed to analyse the outcomes, including evaluation of symptom scores, grading of clinical signs, and assessment of the overall therapeutic response.
Female patients aged between 14 and 35 years were included in this study. Only those with confirmed polycystic ovarian disease (PCOD) based on hormonal assays and ultra-sonographic (USG) findings were selected. Improvement was primarily assessed based on symptomatic relief and the appropriateness of the prescribed remedy as reflected through clinical outcomes. Patients younger than 14 years or older than 35 years were excluded from the study. Additionally, cases of PCOD associated with malignant conditions, metastatic diseases, severe structural abnormalities, or complicated thyroid disorders were omitted from the analysis. Each case was followed for a minimum duration of 3 to 6 months. During the treatment period, progress was carefully compared with the patient's prior clinical condition and previous treatment history.
The evaluation was based on the reduction of clinical symptoms, improvement in general health, psychological well-being, and normalization of menstrual patterns. These observations are detailed in Table 1. All included cases were assessed for parameters such as age, clinical presentation, etiological factors, types of menstrual irregularities, acute prescriptions used, and overall treatment effectiveness. This data is presented in Table 1 and Table 2. To analyse the difference in clinical outcomes before and after the Homoeopathic intervention, statistical methods were applied. An "F-test" was used to evaluate the variance in symptom severity and improvement indices before and after treatment. Additionally, a "T-test" was conducted to determine the significance of changes in symptom scores pre- and post-treatment. The statistical outcomes are compiled and presented in Table 2.
|
Category |
No. of. Patients |
Percentage (%) |
|
According to Age group |
||
|
14-25 |
8 |
80.00 |
|
26-35 |
2 |
2.00 |
|
According to Symptoms |
||
|
Amenorrhea |
9 |
90.00 |
|
Stoutness |
6 |
60.00 |
|
Hair progress |
6 |
60.00 |
|
Asymmetrical menstruation |
8 |
80.00 |
|
Shady spots of skin |
6 |
60.00 |
|
Acne |
8 |
80.00 |
|
According to Potency |
||
|
200 potency |
5 |
50.00 |
|
1M potency |
3 |
30.00 |
|
50 Millesimal |
2 |
20.00 |
|
Intensity of the symptoms: |
Before |
After |
|
Amenorrhea |
3 months once |
Consistent |
|
Stoutness |
Increases |
Reduced |
|
Hair progress |
Persist 3 months Twice in month |
Intermittently |
|
Asymmetrical menstruation |
3 months once |
Consistent |
|
Shady spots of skin |
Persist 3 months |
Nil |
|
Acne |
3 months once |
Rarely seen |
|
According to Symptoms: |
Pre-test score |
Post –test score |
|
Amenorrhea |
8 |
0 |
|
Stoutness |
7 |
2 |
|
Hair progress |
7 |
1 |
|
Asymmetrical menstruation |
9 |
0 |
|
Shady spots of skin |
8 |
0 |
|
Acne |
8 |
1 |
Table 1: Illustration of patient blowout across clinical categories
The outcomes of Homoeopathic treatment in ten cases of Polycystic Ovarian Disease (PCOD) are presented here, with each case being followed for a minimum duration of three months. The results were documented based on symptomatic improvement and verified through clinical comparisons before and after treatment. The effectiveness of Homoeopathic remedies was assessed by analysing the presenting symptoms and selecting appropriate potencies in accordance with individualized prescribing. [16, 17] Most patients showed significant clinical improvement, particularly in terms of symptom resolution and overall well-being. [18] However, a small number of cases with severe pathology required additional interventions such as laser surgery. [19] As noted by Dr. Samuel Hahnemann in the footnote to Aphorism 94 of the Organon of Medicine, special consideration must be given to factors such as pregnancy, infertility, childbirth, miscarriage, lactation, and the phases of the menstrual cycle when treating chronic diseases in women.
|
According to results |
No. of. Patients |
Percentage (%) |
|
Marked improvement |
7 |
70.00 |
|
Moderate improvement |
2 |
20.00 |
|
Mild improvement |
1 |
10.00 |
Table 2: Patient categorization according to treatment efficacy
Although contemporary perspectives may differ in sequence or interpretation, as Hahnemann stated in his lesser writings, "I would practically admit for the sake of reconciliation, if it proves useful to some of us" [20]. The grading of outcomes is illustrated in Figure 1 and detailed in Table 2. Among the ten patients observed, seven demonstrated significant improvements in symptoms, two showed moderate improvement, and one exhibited only slight progress. The results of the study, particularly in relation to the miasmatic interpretation of disease, are presented in Table 3 and Figure 1. Homoeopathic remedies were prescribed based on individual miasmatic presentations: Thuja Occidentalis was used in 5 cases (50%), Calcarea carbonica in 2 cases (20%), Natrum Muriaticum in 2 cases (20%), and Oophorinium in 1 case (10%). The distribution and outcome of anti-miasmatic remedies are summarized in Table 3, supporting the conclusion that anti-miasmatic treatment plays an effective role in the management of Polycystic Ovarian Disease.
|
Type |
No. of. Patients |
Percentage (%) |
|
Miasm |
||
|
Psora |
2 |
20.00 |
|
Sycosis |
7 |
70.00 |
|
Psora-sycosis |
1 |
10.00 |
|
Anti-Miasmatic remedies |
||
|
Thuja Occidentalis |
5 |
50.00 |
|
Calcarea carbonicum |
2 |
20.00 |
|
Natrum Muriaticum |
2 |
20.00 |
|
Oophorinium |
1 |
10.00 |
Table 3: Representation of miasmatic types and corresponding anti-miasmatic remedies
According to the statistical analysis, the significance of symptom reduction before and after treatment was evaluated using the formula: d = ∑d / n, where d represents the difference in symptom scores and n is the number of observations. The calculated t-value was compared against the critical values for t with (n–1) degrees of freedom. For 29 degrees of freedom, the critical t-values are 2.045 at the 5% significance level and 2.756 at the 1% significance level. In this study, the observed t-value was 16.1, which is significantly higher than both critical values. As a result, the null hypothesis was rejected, indicating a statistically significant improvement in symptoms following Homoeopathic treatment. These findings provide strong evidence supporting the effectiveness of Homoeopathic management in reducing the intensity of symptoms in patients with Polycystic Ovarian Disease.
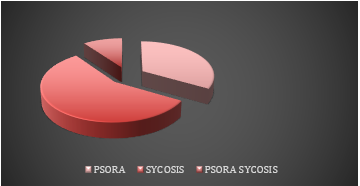
Figure 1: Distribution of patients based on miasmatic classification
A total of 10 cases were selected through random sampling, adhering strictly to inclusion and exclusion criteria. The cases were carefully examined and included based on a comprehensive assessment of presenting symptoms, which were then correlated with Materia Medica and Repertorization findings [15]. Each patient was followed for a minimum duration of 3 to 6 months. The study was subjected to statistical evaluation, and the results were derived through consistent clinical observation and analysis. Through the investigation of symptom patterns and improvement in scoring criteria, the study found that Homoeopathic treatment played a significant role in managing Polycystic Ovarian Disease (PCOD). According to the principles of Homoeopathy, Hahnemann emphasized that in chronic diseases, it is vital to trace and consider underlying causes—whether mental, emotional, or physical—and to observe the timing, modality, and associated symptoms before, during, and after the appearance of complaints [19,20].
The origin sources of chronic conditions often originate from deep-seated, persistent miasms. These miasms may be triggered by latent infections or prolonged stressors, leading to the manifestation of chronic pathology [20, 21]. Homoeopathy aims to gently stimulate the healing response, often pushing latent Psora into remission and restoring a semblance of health, particularly in young and resilient individuals. As described by Hahnemann, this process reflects the curative nature of Homoeopathic remedies when appropriately selected [22,23]. In this study, the majority of cases were associated with the dominant miasm sycosis. A comparative statistical analysis of symptom scores and miasmatic classification revealed a significant reduction in post-treatment scores when compared to pre-treatment values [24]. This numerical evaluation supports the conclusion that Homoeopathic treatment particularly anti-miasmatic prescribing can offer effective relief in managing both the symptoms and the underlying syndrome of Polycystic Ovarian Disease.
Jana, Balaram. Gynaecology and Obstetrics. B. Jain Publishers, 2002.
Sheeba S, Santhi Serene Sylum V, Gokul Krishna K, Dhanya S.S, Sundarapandiyaraj S, Nisha Gopinath and Sruthi Krishna. Efficacy of Homeopathic Medicine in Treatment of PCOD: A Retrospective Study. Chinese Journal of Evidence-Based Medicine. 2024;20(1).
Arulkumaran, Sabaratnam, William Ledger, Lynette Denny, and Stergios Doumouchtsis, eds. Oxford textbook of obstetrics and gynaecology. Oxford University Press, 2019.
Bhargava, Sumeet, and Satish Kumar Bhargava. Textbook of color doppler imaging. Jaypee Brothers Medical Publishers, 2019.
Sheeba, S., K. Gokul Krishna, Premalata B. Rotti, T. Madhavi Chandra, and Fathima Shahunaj. "GYNECOLOGICAL DISORDERS IN PREGNANCY: ANATOMY, PATHOPHYSIOLOGY, AND CLINICAL PERSPECTIVES."
Bennett, Phillip, and Catherine Williamson. Basic Science in Obstetrics and Gynaecology E-Book: Basic Science in Obstetrics and Gynaecology E-Book. Elsevier Health Sciences, 2014.
Dhanya, S., Sheeba, S., Sylum, V. S., & Saheena. (2024). Insights and perspectives on polycystic ovarian syndrome: A narrative review. Journal of Nonlinear Analysis and Optimization, 15(1), Article No. 6.
Dutta, D. C., and Hiralal Konar. "DC Dutta's textbook of gynaecology including contraception." (2013).
Bhargava, V. L. Textbook of Gynaecology. Ane Books Pvt Ltd, 2009.
O'dowd, Michael J., and Elliot Elias Philipp. The history of obstetrics and gynaecology. CRC press, 2000.
Mudaliar, A. L. Mudaliar and Menon's clinical obstetrics. Orient Blackswan, 2005.
Sheeba, S., S. V. Sandhya, D. Genesis Marin Gold Pushpam, K. Gokul Krishna, V. Santhi Serene Sylum, and E. Arun Kumar. "EVALUATION OF HOMOEOPATHIC REMEDIES IN THE MANAGEMENT OF PCOD: A RETROSPECTIVE ANALYSIS."
Kurjak, Asim, and Jose Bajo Arenas. Donald school textbook of transvaginal sonography. JP Medical Ltd, 2018.
Boericke, William. New manual of homoeopathic materia medica and repertory. B. Jain Publishers, 2002.
Kent, James Tyler. Repertory of the homoeopathic materia medica. B. Jain Publishers, 1992.
Hahneman, Geoffrey Mark. The Muratorian fragment and the development of the canon. Oxford University Press, 1992.
Nash, Eugene Beauharnais. Leaders in Homoeopathic Therapeutics: With Grouping and Classification. B. Jain Publishers (P), 2008.
Kent, James Tyler. Lectures on homoeopathic philosophy. B. Jain publishers, 2003.
Roberts, Herbert A. The principles and art of cure by homoeopathy: a modern textbook. B. Jain Publishers, 2002.
Sheeba S., Gokul Krishna K., Dhanya S.S., Sheeba C.S., Sundara pandiya raj S., & Krishna S. (2023). Investigating the Role of Homeopathy in Managing PCOS Through a Retrospective Analysis with Miasmatic Considerations. International Neurourology Journal, 27(4). https://doi.org/10.5123/inj.2023.4.in70
Hahnemann, Samuel. The Chronic Diseases: their peculiar nature and their homoeopathic cure. Vol. 1. C. Ringer & Company, 1896.
Samuel, Hahnemannn. "Organon of Medicine. fifth and sixth edition. New delhi: Kuldeep Jain, B." (2004).
Hahnemann, Samuel. The lesser writings of Samuel Hahnemann. William Radde, 1852.
Sheeba S, Sylum VSS, Reghu R, Sanju SSS, Ramya S. Clinical Study to Determine the Effectiveness of Pulsatilla Nigricans in the Management of Hypothyroidism with PCOD. Open Access Journal of Gynecology. 2025;10(1):000299. doi:10.23880/oajg-16000299