Sergey Suchkov1,2,3,4,5,6,7*, Afaf El-Ansarya8,9, Amina Al-Haidan8, Veronika Polyakova7, Laila Al-Ayadhi9,10, Lydia Kadyrova4 and Wail M. Hassane11
1 The Russian Academy of Natural Sciences (RANS), Moscow, Russia
2 Department of Clinical Allergology & Immunology of the Russian University of Medicine,
Moscow, Russia
3 New York Academy of Sciences, USA
4 EPMA, Brussels, EU
5 PMC, Washington, DC, USA
6 SPM, Tokyo, Japan
7 The University of World Politics & Law, Moscow, Russia
8 Autism Center, Lotus Holistic Alternative Medical Center,, Abu Dhabi, UAE
9 Central Research Laboratory, Female Campus, King Saud University, Riyadh, Saudi Arabia
10 Autism Research and Treatment Center, Riyadh, Saudi Arabia
11 Department of Biomedical Sciences, University of Missouri Kansas City, School of Medicine
*Correspondence: Sergey Suchkov, Department of Clinical Allergology & Immunology of the Russian University of Medicine, Moscow, Russia, E-mail; ssuchkov57@gmail.com
Citation: Sergey Suchkov, Afaf El-Ansarya, Amina Al-Haidan, et al. “Paving the Way & Translating PPH Resources towards Autism-related Care.” Immunol Res Immunother (2023): 103. DOI: 10.59462/IRIT.1.1.103
Received date: 5 December ,2023; Accepted date: 10 December,2023 Published date: 28 December, 2023
Copyright: © 2023. Suchkov S This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
The link that might exert reliable control over morbidity, mortality and disabling rates as well as significantly optimize the efficacy of autism spectrum disorders (ASDs) treatment for those who had fallen ill and for persons-at-risk is Personalized & Precision Medicine (PPM). Since there are significant molecular and neurobiological overlaps among ASD-related clinical phenotypes, targeted and/or smart (intelligent) treatments developed for a specific ASD subtype, may be helpful in ASD of unknown etiology. Recent changes in diagnostics criteria have contributed to the broadening of the ASDs and left clinicians ill-equipped to treat the highly heterogeneous spectrum that now includes toddlers and children with sensory and motor issues. And the biomarker discovery and thus the biomarker-driven drug design have the potential to tailor therapeutic interventions to fit individualized ASD-related conditions in order to receive maximum benefits. This review summarizes the current advances in ASD biomarkers and discusses the potential implementation of biomarkers in PPM-affiliated areas in the context of ASDs, whilst stressing the impact of PPM as the Science and ART and illustrating application of the different tools of the next step generation at the population, community and individualized levels.
Keywords: Autism spectrum disorders • Biomarkers • Personalized precision medicine • GABA • Glutamate • Mitochondrial dysfunction • Gut microbiota.
PPM is a kind of the approach to healthcare that aims to tailor medical treatments and interventions to individual patients and/or persons-at-risk. The approach is based on the idea that every client's genetic makeup, lifestyle, and environmental factors play a critical role in their health outcomes and response to treatments. By considering a patient's lifestyle, environment, and medical history, doctors can develop a treatment plan know as clinical decision, that is tailored to the individual patient or a person-at-risk [1]. In reality, we would need to identify the biomarkers that can be used to assess the functioning of the crucial and ASD-driven pathways as well as suggesting how those biomarkers could guide novel treatment strategies to correct these biochemical abnormalities in order to improve core and associated symptoms of ASD. In this context, PPM is a medical paradigm that emphasizes systematic use of individual patient/person-at-risk information to optimize that patient's health care, particularly in managing chronically diseased or pre-illness conditions. For most of the practitioners, the above-mentioned sequential clinical decision making is known as an adaptive treatment strategy (ATS) to be based on the valuable and validated biomarkers [2]. Meanwhile, an ASD Treatment Plan is a personalized and structured approach to address the unique needs of individuals with autism to improve the client’s quality of life. In this sense, the assessment and identification of relevant physiological alterations and targeted intervention are more likely to produce positive treatment outcomes.
As such, current evidence indicates the utility of an approach based on PPM, rather than treatment targeted to all that may not always be beneficial [3] A variety of potential biomarkers, from the level of genes and proteins to network-level interactions, is currently being examined. A good understanding of the underlying mechanism for various clinical symptoms can lead to identification of potential and valuable biomarkers, and development of effective drugs to treat ASD-related conditions [4]. Effective treatment and management for individuals with ASD is only starting to be uncovered, but we believe the articles within this volume provide insight and a starting point for the evolution of rational and optimal treatments for individuals with ASD [5]. Recent research has focused on identifying specific biological abnormalities in ASDs that can provide clues to diagnosis and treatment. Biomarkers are an objective way to identify and measure biological abnormalities for diagnostic purposes as well as to measure changes resulting from treatment. Many of these biomarkers have promising preliminary evidence for prenatal and post-natal pre-symptomatic risk assessment, confirmation of diagnosis, subtyping, and treatment response. And thus PPM-driven approach may be optimal for understanding and treating each individual with ASD based on their individual unique characteristics [6].ASD is most often triggered by a range of different genetic variants that interact with environmental.
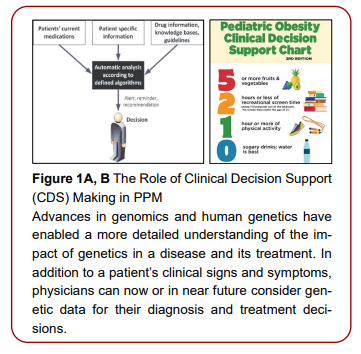
These genomic variants contribute to ASD by interacting with each other, along with nutritional and environmental factors. And a clinical decision support (CDS) tool that specifically focuses on variants and pathways that have been associated with neurodevelopmental disorders, is developed being based on biomarker- and target-dependent strategies to help develop a targeted, personalized prevention and intervention strategy for each ASD compromised child [7]. The latter helps the practitioners identify and develop personalized and genomically targeted treatment plans to secure significant improvements in socialization and overall increased ability to function in those children. As you might see from the above-mentioned, an autism module would have to be added to an existing computer decision support system (CDSS) and health IT-driven datasets to facilitate adherence to recommended guidelines for screening for ASDs, particularly, in primary care pediatric clinics. CDSS can serve as the foundation to support a wide range of clinical and pre-clinical applications ranging from decision support systems for practicing physicians to construct interdisciplinary clinical diagnostic monitoring platform for the daily ASD-related clinical manipulations and practice as a whole [8].In this context, improved patient (or persons-at-risk) outcomes with the application of the biomarker-driven targeted tests must consider not only increased survival or quality of life, but also improved Clinical Decision Support (CDS) & Making, leading to the avoidance of unnecessary therapy or toxicity (Figure 1A, and Figure 1B)
CDS systems are AI based automated systems developed for supporting and the accuracy of CDS-
making processes, have an effect on the rate of routine screening for ASD in general pediatric practice. In this sense, let us stress that during initial diagnostic and treatment planning visits for children with autism spectrum disorder, the level of shared decision-making (SDM) determined by parent and provider reports is usually higher than the level of SDM determined by objective observation using a standard validated rating method. Interventions that may improve SDM in these settings include decision aids, which can facilitate SDM and empower providers and parents to work together to develop a treatment plan that is best suited for the child and family’s needs. In this context, we would stress that a genomic clinical decision support (CDS) tool that specifically focuses on variants and pathways that have been associated with neurodevelopmental disorders was used in this pilot study to help develop a targeted, personalized prevention and intervention strategy for each child. In addition to an individual's genetic makeup, each patient's personal history, diet, and environmental factors were considered.
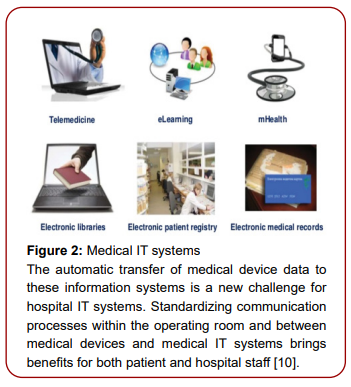
The interpreted genomics tool helped the treating clinician identify and develop personalized, genomically targeted treatment plans. Utilization of this treatment approach was associated with significant improvements in socialization and verbal skills, academic milestones and intelligence quotient (IQ), and overall increased ability to function in these children, as measured by autism treatment evaluation checklist (ATEC) scores and parent interviews [9]. Who will ASD Patients or Persons-at-risk and their Physicians trust to store and interpret the clinical data collected, harvested and mined? Health care IT does offer a potential solution to surmount those barriers (Figure 2) [10]. As a result, a Patient or a Person-at-Risk becomes a data carrier (Figure 3) In line with clinical heterogeneity observed among patients diagnosed with ASD, the genetic architecture of ASD is also highly complex and variable. Currently, ASD is diagnosed according to behavior-based criteria that overlook clinical and genomic heterogeneity, thus repeatedly resulting in failed clinical trials. Now over 1,000 genes might contribute to the risk of ASD, including genes with high penetrance for ASD rarely disrupted in the general population and typically resulting in monogenic ASD-related conditions, as well as those contributing to more polygenic forms of ASD in which additive effects derived from common variants can be determinant.
To date, around 100 genes are confidently associated with ASD risk. Nevertheless, individual genes and variants associated with elevated risk of developing ASD typically account for a very small proportion of the cases. Consequently, genes that are broadly accepted by the professional medical community to be associated with the risk of ASD (such as CUL3), do not always reach
significance in large-scale GWAS [11]. Anyway, the true role of genetics in and the impact of genetic testing following an ASD diagnosis, warrant further investigation. ASD is heterogeneous with high individual complexity, and new findings related to systemic alterations in ASD should be considered when attempting to optimize ASD-related patient health. Meanwhile, a combination of genomic and phonemic (phenotypic) biomarkers are becoming of great significance to be translated into the daily PPM-driven ASD-related clinical practice (Figure 4).to predict risks of the chronification and thus of disabling with much more and reliable accuracy. Due to the extremely diverse genetic phenotype of patients, PPM may be a future avenue for maximally effective treatment. A condensed series of genetic tests could be an expedient and cost-effective solution to determining genetic etiology. Alternatively, therapies may be developed to address convergent disease phenotypes that encompass multiple genetic etiologies, such as neuronal hyper-excitability and abnormal synaptic function. Meanwhile, clarification of phenotypic along with genotypic variations within the phenome (Figure 5) will benefit the implementation of the PPM-based platforms aiming at harvesting data from a wide scope of data sources including the hidden ones. Since phenome is considered to be a bridge from genome,

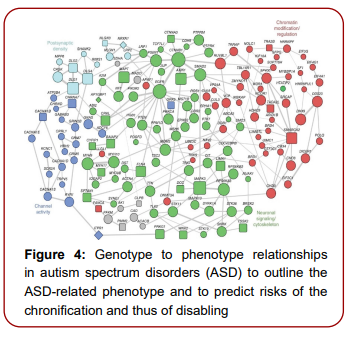
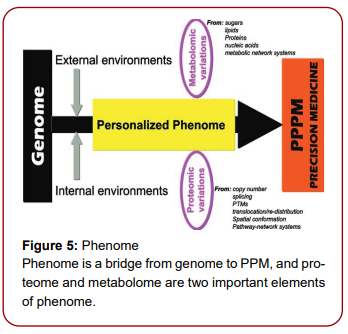
proteome and metabolome, which are two important elements of phenome [12].
In addition, the success of clinical trials that examined specific treatments and outcomes also demonstrated another challenge: the application of consistent and reproducible measures of assessing improvement. Current approaches depend chiefly on behavioral tests that are biased, less consistent, and greatly affected by the “placebo effect” hypothesized that some of the unsuccessful pharmacological and behavioral treatment trials are mostly attributed to the combination of biological and behavioral measures (which are strongly affected by the placebo response) that are utilized as endpoints for the studies.
It is possible that some of the drugs or behavioral interventions would have resulted in further improvements by using a subgroup of ASD patients that were more biologically homogenous and a more consistent and objective biomarker for assessing improvements [13]. Impaired social interaction and communication as well as restricted and repetitive behaviors are the main autistic features. ASD cases are predominantly male, with nearly four males diagnosed with ASD for each female diagnosed; however, the sex ratio seems to decline with severity. While this noticeable sex difference is found in all studied populations, variance in the clinical presentation in females, and probable associated diagnostic biases, require additional investigation. A range of comorbid medical conditions are commonly associated with ASD, such as intellectual disability, sensory hyper or hypo sensitivities, dysibiosis, immune response insufficiencies, epilepsy, anxiety, and sleep difficulties [14].The National Institute of Mental Health (NIMH) Research Domain Criteria (RDoC) initiative was developed to motivate investigators to evaluate diagnostic tools and give more attention for behavioral and neurobiological features that could be targeted to improve our understanding of typical, versus pathological, features. Tools have been established to measure the range of behavioral dimensions characteristic of ASD (e.g., the Social Responsiveness Scale (SRS) and the Childhood Autism Rating Scale (CARS)), and such assessments are being used more widely. Approaches for creating continuous severity scores among individuals diagnosed with ASD have also been developed [15].
The relationship between the neurobiological and neurochemical bases of ASD and altered behavior
In the last decade, social neuroscience as field of research has stressed the contribution of neuroanatomical brain regions in the impairment of social behavior, as core features of ASD clinical presentation. This relationship seems to be bidirectional. That is, the ability to show appropriate social behavior skills (i.e., suitable eye contact) affects neurobiological measures. In turn, neurophysiological, neuroanatomical, and neurochemical actions happening in cortical and subcortical brain regions initiate and control an individual’s capability to perceive meaning in rational traits of communication. These skills include interpreting facial expressions, proper use of eye contact, and mutual responsiveness. Most recently, abnormal Cerebellar Development is increasingly thought to contribute to aberrant social and linguistic functions which are hallmarks of ASD [16]. Many neurochemical pathways contribute to the etiology of ASD; nevertheless, it remains unclear how these complexes signaling interact and induce the core symptoms of autism. Despite the large number of studies on neurochemical alterations in autism, additional studies are essential to shed more light on the etiological mechanisms that contribute to the initial neurodevelopmental differences that lead to the substantial heterogeneity of ASD and thus indicate novel strategies for the prevention and treatment of autism through PPM.Neurochemical dysfunctions of numerous neuropeptides and neurotransmitters, including oxytocin, vasopressin, melatonin, vitamin D, opioids, GABA, glutamate, serotonin, dopamine, and acetylcholine, contribute to the etiology of autism. Recently, [21] suggested that altered neurotransmission has a central role in the etiology of ASD.
The excitatory/inhibitory imbalance theory, which involves the synaptopathy of the GABAergic and glutamatergic systems which is related to the impaired social behavior as the core symptom in ASD, and has been validated through the long duration depolarization of neuronal cells in the medial prefrontal cortex of mice. The imbalanced inhibitory/ excitatory neurotransmission induces a marked impairment in social interaction and handling of information [17]. In a translational magnetic resonance spectroscopy [1H] MRS studies on humans with autism and in five mouse models and one rat model of ASD, idiopathic adult ASD recorded lower glutamate levels in the striatum, high affinity GABA transporters, than controls. Mouse models included: mice prenatally exposed to VPA through their mothers, BTBR T+tf/J mice, 15q11-13 patDP mice Shank3 KO mice, Nlgn3R451C KI mice C57BL/6J genetic, and in addition, Nlgn3 KO rats [18]. Several studies have highlighted a relationship between single-nucleotide polymorphisms (SNPs) of GABAA receptors positioned on chromosomes 15q11–q13 and individuals with ASD. However, a latest meta-analysis revealed that SNPs of B3, A5, and G3 subunits of GABAA receptor were not associated with ASD in many populations [19]. This contradict could be explained on the basis that increased GABA production in ASD could compensate for GABA receptor dysfunction. Furthermore, research mentioned above was not based on GABAB receptor dysfunction which have been proved in many studies with ASD [20]. Surprisingly, lower excitatory synaptic transmission and much higher I/E ratio in pyramidal neurons of the developing mouse prefrontal cortex (PFC) lead to impaired social interaction as well as speech abnormalities, which may trigger the etiolopathology of a subgroup of autistic patients.
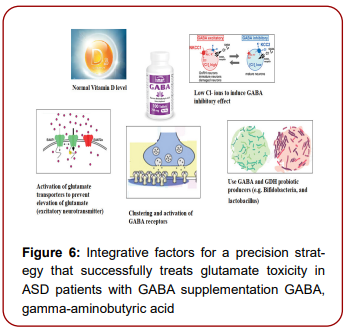
Thus, improvement of excitatory synaptic transmission might be promising for treating particular ASD patients. This might suggest that imbalances in E/I neurotransmission should be targeted by PPM-driven [21]. Afaf El-Ansary (2020) suggested a medical hypothesis through which reversal of imbalanced GABAergic/glutamatergic neurotransmission could be used as a strategy for personalized treatment. This hypothesis integrates the therapy to restore normal GABAergic signaling through GABA supplementation with antioxidant status, vitamin D status, intracellular chloride concentration [Cl−]i, normal gut microbiota, functional glutamate transporters, and active GABA receptors (Figure 6). It is well accepted that insufficiency or deficiency of vitamin D are usually accompanied with much lower activity of glutamic acid decarboxylase, the rate limiting enzyme in GABAergic interneurons together with lower levels of glutamate and glutamine in mouse brain tissue. This suggests that impaired glutamate-glutamine-GABA cycle as a consequence of glutamate excitotoxicity could be corrected through vitamin D supplementation [22]. In relation to ASD patients, reported a significantly much lower vitamin D levels in individuals with autism compared to healthy controls. Vitamin D deficiency was positively correlated with the severity of autistic features. Since vitamin D deficiency is associated with the high incidence of ASD, regular measurement of vitamin D levels in children and adolescents with autism could be a critical precision strategy to correct the imbalance in E/I neurotransmission.
Additionally, because pregnant and lactating women consume more vitamin D than usual (yet are usually vitamin D insufficient), vitamin D status should be recommended as routine test during pregnancy and lactation to provide proper clinical intervention at the proper time. Developmentally controlled intracellular chloride
concentrations ([Cl−]i) are the main factor that contributes to GABA action at GABAA receptors. In immature neurons, GABA signaling mostly induces depolarizing response in the presence of high [Cl−]i, which plays an active role in neurogenesis and synaptic networks; however, in mature neurons, a hyperpolarizing effect of GABA signaling usually occurs under low [Cl−] i concentrations [23]. The K+-Cl− cotransporter KCC2 facilitates the efflux of Cl− from cells and the Na+, K+-2 Cl− cotransporter NKCC1 stimulates Cl− uptake. The reduction in [Cl−]i, which take place during the maturation of neural cells is crucial, resulting in a shift of GABAergic transmission from excitatory to inhibitory, and is under transcriptional and epigenetic control. Reported that oxidative stress or poor antioxidant status caused the GABA neurotransmitter to lose its inhibitory effect and that this dysfunction was concomitant with a marked decrease in the expression of the chloride cotransporter KCC2, resulting in much higher [Cl−]i. By treating oxidative processes and scavenging ROS, normal levels of KCC2 and [Cl−]i can be restored [24].
This suggests multiple integrated strategies for treating autistic patients should be considered from a personalized precision perspective. For example, using GABA supplementation to treat autistic individuals suffering from vitamin D deficiency, imbalanced antioxidant/pro-oxidant status, or high [Cl−] i will be ineffective. As might see from the above-mentioned, by using GABA-related approach, the ibiodesigners can target the biomarker directly and measure the impact of the treatment. This will help with the future development of targeted therapies for ASD and provide a pre-early (subclinical) marker of response to aid in the selection of individuals more likely to respond to various treatments and to provide a rational basis for pharmacological treatment of the core social deficits of ASD, providing direct benefit to the patients and even persons-at-risk in the future.
Biomarker–directed personalized precision treatment strategies for ASD
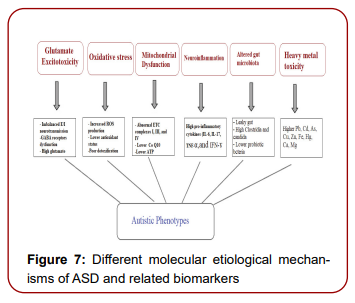
The aim of PPM is to offer the correct treatment at the right time for each patient. Biomarkers are generally defined as a specific variable that is an indicator of normal biological or pathological processes or pharmacological responses to a therapeutic intervention. Biomarkers of ASD may be detected before birth and after diagnosis, and some are expected to respond to precision medicine. Many highly predictive biomarkers of ASD have been detected. Nevertheless, most of these biomarkers are preliminary and their role in the detection and early intervention of ASD prerequisites further investigation [25]. Combining known biomarkers would probably be more effective in the early identification of ASD and thus could guide successful treatments. Biomarkers include measurements of brain function or anatomy (electroencephalogram [EEG], imaging), or proteomic and metabolomics candidates that indicate alterations in immune function, oxidative stress, or neurotransmission. In addition, clinical presentation that are established by direct examination of patients could also be used as markers. Medical (e.g., epilepsy, sleep troubles, altered gut microbiota) and psychiatric comorbidities can guide pharmacological control strategies. Other markers more specific to ASD have a less clearly defined relationship to treatment. Defined autistic features such as impairment in social communication, repetitive behaviors, and linked features among which is abnormal sensory sensitivity (i.e hypersensitivity/hyposensitivity) may represent appropriate treatment targets. The current drive for precision medicine stems from the lack of effective early intervention or treatment strategies and the need to determine the phenotypic and etiological inconsistencies between individuals. This drive aims to target treatments based on understanding of the etiopathological mechanisms of ASD and to combine interventions (or drugs) with diagnostic biomarkers to recruit or exclude patients to precisely manage this disorder. Among these etiological mechanisms are glutamate excitotoxicity, oxidative stress, mitochondrial dysfunction, neuroinflammation, Altered gut microbiota, and heavy metal toxicity.
Figure 3 demonstrates different molecular etiological mechanisms of ASD (Figure7). The main advances in drug treatment of ASD originated from the identification of highly penetrant genes in individuals with autism. Hundreds of ASD risk genes have been identified, and more are anticipated to be identified in the future through larger sample sizes and sequencing of whole the genome [26]. The impact of these discoveries lies in their capability to find a probable fundamental link between a gene and principal cellular signaling pathways that are related to the clinical presentation of autism. Based on this link, specific biological processes, such as oxidative stress, neuroinflammation, receptor signaling, and glutamate excitotoxicity, could be targeted rather than individual gene products, and these intervention methods could apply to larger patient groups with similar clinical presentations [27]. Multimodal biomarkers such as the combination of resting-state EEG and fMRI, may have better prognostic and predictive value when compared to single modality biomarkers. For example, deviations in gamma band oscillations possibly demonstrate either higher excitatory (e.g., glutamatergic) or lower inhibitory (e.g., GABAergic) signaling. More information on glutamate and GABA levels resulting from MRS may assist in the understanding and interpretation of EEG scores. It would be highly useful to specify whether a glutamate (receptor) antagonist,
or GABA agonist would be highly recommended for a given individual. Additionally, a clear understanding and assessment of a patient’s cognitive ability across different domains is essential for ASD individuals and their families and caregivers to agree to future medical interventions. Longitudinal designs with no less than three-time intervals that simultaneously measure alterations in clinical presentation and neurocognitive, functional, and anatomical courses to find out the prognostic value of biomarkers are desirable. As large clinical trials have tried to target GABAergic (arbaclofen) and glutamatergic (memantine) systems, markers representing the activity of both systems, as evaluated by MRS or other proxy markers such as EEG gamma band activity, would be particularly useful [28].
Additional markers that may be appropriate for early intervention could include immune system-related biomarkers that frequently affected in, such as whole-blood serotonin, genetic polymorphisms that influence serotonergic transporters, or serotonin ligand markers on positron emission tomography. In the context of personalized precision medicine, understanding the persistent changes in 5-HT signaling in ASD could be a critical prerequisite for successful treatments with selective serotonin reuptake inhibitors (SSRIs). SSRIs block 5-HT reuptake through pharmacologic inhibition of the serotonin transporter, increasing extracellular levels of 5-HT. Improved extracellular levels of 5-HT with SSRIs mends symptoms in some individuals with ASD, while it is not useful in others. For example, only approximately 35% of children and adolescent with ASD demonstrate lower irritability, repetitive behavior, and inappropriate communication and hyperactivity when receiving SSRI treatment. While the reason for this difference in response is still unclear, one potential explanation of the inadequate or absent therapeutic efficiency of SSRIs in some individuals with ASD is that these patients already have elevated extracellular 5-HT. For example, these nonresponders could have hypofunctional serotonin transporter (SERT) gene variants and consequently have higher 5-HT levels extracellularly, making additional block from medications useless [29,30]. Approximately 5% of individuals with ASD have a mitochondrial disease and 30–80% display some degree of mitochondrial dysfunction (Mtd). Some blood variables, such as ammonia, aspartate aminotransferase (AST), and creatine kinase, are commonly used biomarkers for identifying mitochondrial dysfunction in ASD, but some of them require more studies to be confirmed. Lactate dehydrogenase, lactate oxidase, pyruvate kinase and hexokinase, Na+/K+ ATPase, Caspase-3 and Caspase-7 are biomarkers related to mitochondrial dysfunction that can help discriminate between ASD patients and healthy controls [31].Overall, identification of mitochondrial dysfunctions as an etiological mechanism in individuals with ASD is very promising from the precision medicine perspective since these children may respond differently to specific treatments depending on the type of dysfunction.
Elevations in levels of proteins, lactate, pyruvate and even white blood cells were confirmed in the cerebrospinal fluid of patients with mitochondrial dysfunction and individuals with ASD. In addition, MtD and oxidative stress may clarify the known 4:1 male/female ratio in autism due to increased susceptibility of males to both dysfunctions. Biomarkers related to mitochondrial dysfunction have been recorded, but they appear generally underutilized regardless of the available treatment interventions [32]. From a clinical perspective, CoQ10 deficiency is well-recognized and could be both primary and secondary. In the primary group, biallelic mutations in the genes encoding CoQ10 synthetic pathway enzymes result in significantly diminished levels of CoQ10 concomitant with a diversity of clinical presentations; therefore, supplementation with CoQ10 may be effective in these patients. Deficiency of CoQ10 has also been recorded in a large number of patients with respiratory chain deficits, but supplementation with CoQ10 in this group has been of inadequate usefulness [33]. showed promising results from activating complex I, complex IV, and citrate synthase by administrating selected mitochondrial supplements, such as coenzyme Q, fatty acids, folate, and vitamin B12. Therefore, understanding the etiological mechanisms of mitochondrial dysfunction in ASD could be essential for identifying new therapeutic targets of autistic features [34]. A recent study evaluated mitochondrial energy generation in a BTBR rodent model of ASD. The authors examined alterations in mitochondrial morphology, which can directly influence mitochondrial bioenergetics-related function.
They reported that BTBR mice had abnormal mitochondrial function demonstrating more scrappy mitochondria than C57BL/6J healthy controls. Consistent with the increase in mitochondrial fragmentation, they found that two fission proteins, pDRP1S616 and pMFFS146, were activated and phosphorylated in BTBR mice. In addition, studied electron transport chain (ETC) complex activity and mitochondrial morphology measurements in fibroblasts obtained from 18 individuals with ASD and 4 healthy controls. In the ASD patients, symptom severity was measured by the SRS and Aberrant Behavior Checklist (ABC). Mixed-model regressions indicated that abnormal mitochondrial morphology was concomitant with the activity of ETC complexes I, III and IV. When compared with individuals with classic mitochondrial illnesses where ETC activity is much lower, some patients with ASD have heightened ETC activity. An increase in ETC complex IV activity was first described in ASD through muscle biopsy and later ascertained in other tissues, such as fibroblasts, buccal epithelium, brain and lymphoblastoid cell lines (LCLs). Since ETC complex IV is the mitochondrial complex responsible for oxygen consumption, increases in ETC complex IV activity lead to markedly higher oxygen consumption or increased mitochondrial respiration. An LCL model in a subset of ASD individuals found a 200% elevation of mitochondrial respiration compared to control LCLs [35]. Most ETC complexes (I, III, and IV) transport protons across the inner mitochondrial membrane to produce a proton gradient that drives ETC complex V, also known as ATP synthase, to produce ATP. The ETC is the major source and target of reactive oxygen species (ROS), such as oxygen radicals. Oxidative stress occurs when the amount of ROS become increased to the point that they affect normal ETC function. To decrease ROS, mitochondria leak protons back across the inner mitochondrial membrane, essentially reducing the proton gradient and decreasing mitochondrial efficiency. Interestingly, LCLs from individuals with ASD with higher respiratory rates are associated with increased proton leakage, uncoupling of the respiratory chain and superoxide elevation in the mitochondrial compartment.
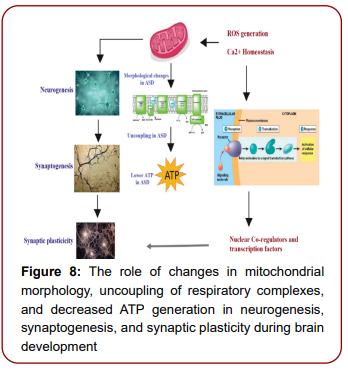
Consistent with this finding, ETC complex I and IV activity were relatively dissociated in buccal epithelium from individuals with ASD, suggesting an uncoupling of the respiratory chain [36]. Similar to mitochondrial dysfunction in ASD, neurogenesis could also be greatly affected. Of all cell types in the CNS, neurons have the highest energy demands. The majority of ATP generated in the CNS is usually used to maintain neuronal excitability and overall synaptic function. To maximize local energy release, mitochondria can be attached to dendrites and synapses to produce ATP, thus stimulating vesicle recycling during neuronal action. However, in addition to postmitotic neurons, mitochondrial oxidative phosphorylation might also play a critical role during neurogenesis. Taken together, mitochondrial dynamic dysfunctions and alterations in mitochondrial morphology or impaired ETC oxidative phosphorylation bioenergetics could have profound effects on physiological neurogenesis and on the proper establishment of neuronal function in the brains of ASD patients [37]. (Figure 8) A ketogenic diet (KD), which is a high-fat, low-carbohydrate and low-protein diet, is known to reduce autistic behaviors in both humans and rodent models of ASD. Interestingly, supplementation of BTBR mice with a KD amends both mitochondrial function and morphology. Furthermore, a KD decreased pDRP1S616 levels in BTBR mice, probably involved in the repair of mitochondrial morphology. These data provide additional proof that impaired mitochondrial energy-generation related functions and mitochondrial fragmentation may be considered as etiological mechanisms of ASD which can be reversed with KD treatment as a form of personalized precision medicine. From the bioenergetics perspective, a KD has a positive effect on energy metabolism.
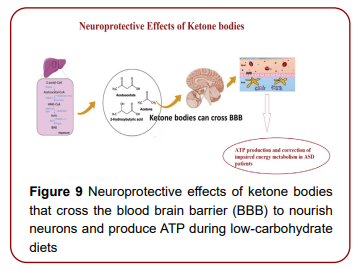
For example, it increases the levels of adenosine triphosphate (ATP) and enzymes associated with mitochondrial energy generation. Acetyl-CoA, a product of fatty acid oxidation, is transformed to ketone bodies through the catalytic activities of D-β-hydroxybutyrate dehydrogenase, acetoacetate succinyl-CoA transferase, and acetoacetic-CoA-thiolase enzymes. Ketone bodies, such as β-hydroxybutyrate, acetoacetate, and acetone, serve as energy compounds in case of starvation, and are capable to cross the blood–brain barrier (BBB) to nourish the brain (Figure 9) [38]. These molecules also help to prevent transitions in mitochondrial permeability and reduce reactive oxygen species (ROS). Thus, ketone bodies have neuroprotective effects on the central nervous system (CNS). Multiple studies have focused on change in the gut microbiota as a risk factor in individuals who are genetically predisposed to ASD. Breastfeeding is associated with a lower risk of ASD if continued for 6 months, while formula-fed infants show a higher amount of Clostridium difficile in the gut [39]. Furthermore, C. difficile has been hypothesized to be a potential risk factor for ASD, supported by a study in which children with regressive autism were treated with a 6-week oral course of vancomycin (an antibiotic used against C. difficile), which resulted in a significant improvement of both neurobehavioral and gastrointestinal symptoms. However, relapsing gastrointestinal and neurobehavioral symptoms occurred gradually after treatment interruption, possibly because the spores of C. difficile were resistant to vancomycin and could turn into infective forms later [40]. From the precision medicine perspective, the use of probiotics as a treatment strategy for ASD be tested,
considering the presence/absence of GI problems. (2020) suggested that ASD children with and without comorbid GI problems could represent two different groups and that probiotic interventions could potentially result in different effects, likely due to the distinctive targeted microbiota. Previous studies have already suggested that differences in gut microbiota are independent of GI dysfunction. suggested that larger and well-designed studies are still needed before it can be concluded whether microbial composition may stratify ASD children without GI problems. A positive impact of probiotics on autism severity in children without GI problems supports the contribution of the microbiota-gut-brain axis as an etiological mechanism of this ASD subgroup. Specifically, probiotic supplementation, acting on dysbiosis, could relieve pain and enteroception caused by GI problems and, accordingly, could improve the multisensorial integration process, which in turn is affected by averse enteroceptive stimuli in dysbiotic patients. Moreover, dysbiosis could impact neurotransmitters that play a role in sensory developmental pathways. Recently, difficulties in multisensory processing have been related to serotoninergic neurotransmission, and serotonin levels are controlled by the gut microbiota. Thus, we hypothesize that probiotics could ameliorate sensory abnormalities by restoring the serotoninergic system, which also works to reduce GI dysfunction comorbidities [41]. Based on the above findings, the therapeutic effects of probiotic supplementation on the NGI and GI groups of autistic children may be due to different mechanisms.
Thus, each medication is likely to benefit only a subgroup of patients within the spectrum, which could be used to ascertain the importance of biomarkers for personalized precision medicine. Understanding the mechanism behind the positive effect of probiotic treatment on both GI and NGI children would greatly facilitate the identification of ASD subjects who can respond to probiotic supplementation regardless of the presence of comorbid GI dysfunction and GI inflammatory grade. To our knowledge, selection of the proper probiotic could be based on the presence or absence of imbalanced GABA/Glu, hyperserotonemia, and depletion of neuropeptides or metabolites (all ASD biomarkers). It is well known that germ-free (GF) animals have much lower brain levels of glutamine (involved in the production of GABA and Glu), tyrosine (a precursor of dopamine and noradrenaline), and tryptophan (a precursor of 5-HT). For example, in the case of ASD patients with glutamate excitotoxicity, administration of Lactobacillus rhamnosus is recommended, as it induces GABAA and GABAB receptors in specific brain regions, accompanied by declines in anxiety and depression-associated behaviors. Collectively, these results suggest that L. rhamnosus is a psychoactive bacterium that is effective in correcting the etiological mechanism of E/I imbalance in ASD. Based on these results, the application of standard clinical neurodiagnostic practices (e.g., MRI), translational opportunities (probiotic supplementation), and regular assessment of related biomarkers (Glx, tNAA, GABA, and GABA receptors) could greatly benefit the field of personalized precision medicine [42]. Hyperserotonemia may also be a biomarker of ASD. Some treatments involving microbial management have potential, including those involving probiotics or fecal transplant. Mice administered Lactobacillus reuteri demonstrate improvements in the GI tract and behavioral alterations. Trials evaluating the role of other probiotics proved that a probiotic mixture of Lactobacilli and Bifidobacteria, particularly L. acidophilus, L. plantarum, L. helveticus, L. paracasei, B. breve and B. lactis, can improve GI symptoms and quality of life in ASD patients and identified significant associations between the microbiome, 5-HT, and gastrointestinal dysfunction in ASD. Findings in humans, however, have been limited, and large prospective trials are needed.
Conclusion
There are no drugs approved that treat the core symptoms of ASD. The recent hypothesis that multiple etiological and pathophysiological mechanisms are involved in ASD makes PPM the most recommended approach for successful treatment and intervention strategies for individuals with ASD [43]. Additionally, a complete understanding of an individual’s cognitive, social, and sensory profiles and the relationship between the treatment outcome measures of these profiles (CARS, SRS, and sensory profile) and the severity of the clinical presentation in ASD could greatly benefit patients with ASD; their families may be more likely to accept future PPM-driven trials if these trials were able to accurately provide prognoses for their ASD children. Currently, there are no medications available to completely cure ASD. However, the identified molecular biomarkers are being evaluated for developing and advancing therapeutic drug development strategies. But, in ASD, interventions are most efficient and successful if they commence as early as possible; however, diagnosis often occurs late, partly because the diagnosis of ASD is primarily based on recognizing autistic behaviors that may not appear until the disorder is already clinically presented. In this sense, clustering of patients with similar etiologies and neurodevelopmental symptoms may allow mechanism-based PPM-driven strategies for these conditions. Similarly, advancements in physical interventions and virtual reality approaches to meet each individual's unique requirements may complement understanding of genetic pathobiology and further improve the ASD management [44].
Based on this delay, identifying biomarkers that indicate at-risk children during the presymptomatic period could greatly facilitate early diagnosis, confirm behavioral abnormalities, classify patients into subgroups, and predict personalized precision treatment strategies related to the biomarkers in different subgroups Recently, unsuccessful clinical trials were attributed to theoretical and methodological concerns related to the translatability of research data from animal models to humans, the design of different clinical trials, placebo effects, and objective measures of clinical trial outcomes. In the future, translatable progressive multidisciplinary joint integrated interventions are required to overcome these concerns. Meanwhile, to identify potential drugs for repurposing to effectively treat ASD core symptoms, we would have to re-orient our focus on ASD-related risk genes within networks of protein-protein interactions of gene products, whilst defining the ASD networks from network-based analyses, and identifying pre-approved drugs known to interact with proteins within this network. The drugs mentioned would have to act on ASD-related biological systems, indicating that these drugs could effectively treat ASD core symptoms [45]. The understanding of the causative relationship between various network-related and genetic perturbations on one hand and ASD clinical signs on the other one, may further improve our understanding of the key mechanisms involved and thus help to develop promising biomarkers for efficient screening of patients and/or persons-at-risk at earlier stages of child development and for potential drug development. In this context, a person-centered approach for pre-early prediction and cure of ASD patients is an aspirational goal, and recent advances in understanding human genetic and phenotypic biomarker targets and complementary therapeutic interventions could help develop effective precision medicine tools in the near future. As you might see, the PPM-driven approach to diagnosis and treatment of ASD, although just beginning, holds great promise for improving the lives of affected individuals. Developing drugs for ASD has been challenging because of a limited understanding of its pathophysiology, difficulties in modelling the disease in vitro and in vivo, the heterogeneity of symptoms, and the dearth of prior experience in clinical development. In this context, ASD biomarker-driven targeted drug development challenges our most sophisticated preclinical models and methods for developing precise translational clinical trial (adaptive) designs and identifying curative therapeutics.
This work was funded through the National Plan for Science Technology and Innovation (MAARIFAH), King Abdulaziz City for Science and Technology, Kingdom of Saudi Arabia (award number:08-MED 510-02).
The authors wish to acknowledge the National Plan for Science Technology and Innovation (MAARIFAH), King Abdulaziz City for Science and Technology, Kingdom of Saudi Arabia (award number:08-MED 510-02).
Author Contributions
AE: Suggested the topic and drafted the manuscript; LA: Carefully revised and has approved the submitted version
Institutional Review Board Statement
This work was approved by the ethics committee of King Khalid Hospital, King Saud University (Approval number: 11/2890/IRB).
Informed Consent Statement
Not applicable
The authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Barberis, Elettra, Shahzaib Khoso, Antonio Sica and Marco Falasca, et al. "Precision medicine approaches with metabolomics and artificial intelligence." Int J Mol Sci 23 (2022): 11269.
Brenner, Benjamin, Emmanouil Papadakis and Ian A. Greer et al. "Assessment‐Based Management of Placenta‐Mediated Pregnancy Complications: Pragmatism Until A Precision Medicine Approach Evolves." Br J Haematol ". 202 (2023): 18-30.
Stenzinger, Albrecht, Ejner K. Moltzen and Eva Winkler et al. "Implementation of Precision Medicine in Healthcare—A European Perspective." J Intern Med 294 (2023): 437-454.
Levin, April R., and Charles A. Nelson. "Inhibition-Based Biomarkers for Autism Spectrum Disorder." Neurother 12 (2015): 546-552
Frye, Richard E., Shannon Rose, Richard G. Boles and Daniel A. Rossignol. "A Personalized Approach to Evaluating and Treating Autism Spectrum Disorder." J Pers Med 12 (2022): 147.
Mesleh, Areej G., Sara A. Abdulla and Omar El-Agnaf. "Paving the Way Toward Personalized Medicine: Current Advances and Challenges in Multi-Omics Approach in Autism Spectrum Disorder for Biomarkers Discovery and Patient Stratification." J Pers Med 11 (2021): 41.
Way, Heather, Grant Williams and Sharon Hausman-Cohen et al. "Genomics as A Clinical Decision Support Tool: Successful Proof of Concept for Improved ASD Outcomes." J Pers Med 11 (2021): 596.
Downs, Stephen M., Nerissa S. Bauer and Chandan Saha et al "Effect of A Computer-Based Decision Support Intervention on Autism Spectrum Disorder Screening in Pediatric Primary Care Clinics: A Cluster Randomized Clinical Trial." JAMA Netw Open2 (2019): e1917676-e1917676.
Freimuth, R. R., C. M. Formea, J. M. Hoffman and E. Matey et al. "Implementing Genomic Clinical Decision Support for Drug‐Based Precision Medicine." CPT: Pharmacometrics & Systems Pharmacology 6 (2017): 153-155.
Pahontu, Raluca, Angela Merzweiler and Gerd Schneider et al. "Micro-and Macrointegration Profiles for Medical Devices and Medical It Systems." In MedInfo pp. 222-226. 2015.
Brueggeman, Leo, Tanner Koomar and Jacob J. Michaelson. "Forecasting Risk Gene Discovery in Autism with Machine Learning and Genome-Scale Data." Scientific Rep10 (2020): 4569.
Pendergrass, Sarah A., Scott M. Dudek and Dana C. Crawford” Visually Integrating and Exploring High Throughput Phenome-Wide Association Study (Phewas) Results Using Phewas-View." BioData Min (2012): 1-11.
Gabis, Lidia V., Raz Gross and Josephine Barbaro. "Personalized Precision Medicine in Autism Spectrum-Related Disorders." Front Neurol 12 (2021): 730852.
DeFranco, Emily, Gilad Gross and Anthony Shanks, et al. "Prenatal Exposure to Anti-D Immune Globulin and Autism Risk: Croen et al." Am J Obstet Gynecol 199 (2008): 322-323.
Yap, Chloe X., Anjali K. Henders and Gail A. Alvares et al. "Autism-Related Dietary Preferences Mediate Autism-Gut Microbiome Associations." Cell 184 (2021): 5916-5931.
van der Heijden, Meike E., Elizabeth P. Lackey, Ross Perez and Fatma S. Ișleyen, et al. "Maturation of Purkinje Cell Firing Properties Relies on Neurogenesis of Excitatory Neurons." Elife 10 (2021): e68045.
Akerboom, Jasper, Nicole Carreras Calderón and Lin Tian et al. "Genetically Encoded Calcium Indicators for Multi-Color Neural Activity Imaging and Combination with Optogenetics." Front Mol Neurosci 6 (2013): 2.
Horder, Jamie, Marija M. Petrinovic and Maria A. Mendez et al. "Glutamate and Gaba In Autism Spectrum Disorder—A Translational Magnetic Resonance Spectroscopy Study in Man and Rodent Models." Transl Psychiatry 8 (2018): 106.
Mahdavi, Manijeh, Majid Kheirollahi and Roya Riahi et al. "Meta-Analysis of The Association Between Gaba Receptor Polymorphisms and Autism Spectrum Disorder (Asd)." J Mol Neurosci 65 (2018): 1-9.
Zhao, Haisheng, Xijing Mao and Cuilin Zhu et al. "Gabaergic System Dysfunction in Autism Spectrum Disorders." Front Cell Dev Biol 9 (2022): 781327.
Sacai, Hiroaki, Kazuto Sakoori and Kohtarou Konno et al. "Autism Spectrum Disorder-Like Behavior Caused by Reduced Excitatory Synaptic Transmission in Pyramidal Neurons of Mouse Prefrontal Cortex." Nat Commun 11 (2020): 5140.
Upadhyaya, Subina, Tiia Stahlberg and Sanju Silwal et al. "Maternal Vitamin D Levels During Pregnancy and Offspring Psychiatric Outcomes: A Systematic Review." Int J Mol Sci 24 (2022): 63.
Succol, Francesca, Hubert Fiumelli and Fabio Benfenati et al. "Intracellular Chloride Concentration Influences the Gabaa Receptor Subunit Composition Nat Commun 3 (2012): 738.
Kim, Ye Eun, and Jaeyun Kim. "Ros-Scavenging Therapeutic Hydrogels for Modulation of The Inflammatory Response." ACS applied materials & interfaces 14 (2021): 23002-23021.
Frye, Richard E., Sarah Vassall, and Gurjot Kaur et al. "Emerging Biomarkers In Autism Spectrum Disorder: A Systematic Review." Ann Transl Med 7 (2019).
Satterstrom, F. Kyle, Jack A. Kosmicki, and Jiebiao Wang et al. "Large-Scale Exome Sequencing Study Implicates Both Developmental and Functional Changes in The Neurobiology of Autism." Cell 180 (2020): 568-584.
Yeo, Michele, Heather Patisaul, and Wolfgang Liedtke. "Decoding the Language of Epigenetics During Neural Development Is Key for Understanding Development as Well as Developmental Neurotoxicity." Epigenetics 8 (2013): 1128-1132.
Deligianni, Fani, Maria Centeno and David W. Carmichael et al. "Relating Resting-State Fmri And Eeg Whole-Brain Connectomes Across Frequency Bands." Fnins (2014): 98767.
Rojas Domínguez, Paulina and Jenny Fiedler Temer. "what do we really know about 5-ht1a receptor signaling in neuronal cells?" (2016).
Hyman, Susan L., Susan E. Levy, Scott M. Myers and Dennis Z. Kuo et al. "Identification, Evaluation, And Management of Children with Autism Spectrum Disorder." PEDS 145 (2020).
Jyonouchi, Harumi, Lee Geng and Shannon Rose et al. "Variations in Mitochondrial Respiration Differ in Il-1ss/Il-10 Ratio-Based Subgroups in Autism Spectrum Disorders." Fpsyt 10 (2019): 406333.
Loomes, Rachel, Laura Hull and William Polmear Locke Mandy. "what is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis." JAACAP 56 (2017): 466-474.
Quinzii, Catarina M and Michio Hirano. "Primary and Secondary Coq10 Deficiencies in Humans." BIFAEU 37 (2011): 361-365.
Cheng, Ning, Jong M. Rho and Susan A. Masino. "Metabolic Dysfunction Underlying Autism Spectrum Disorder and Potential Treatment Approaches." Front Mol Neurosci 10 (2017): 34
Frye, Richard E., Loïc Lionnard and Indrapal Singh, et al. "Mitochondrial Morphology Is Associated with Respiratory Chain Uncoupling in Autism Spectrum Disorder." Transl Psychiatry (2021): 527.
Mormone, Elisabetta, Eugenio Luigi Iorio and Lucrezia Abate et al."Sirtuins And Redox Signaling Interplay in Neurogenesis, Neurodegenerative Diseases, And Neural Cell Reprogramming." Fnins 17 (2023): 1073689.
Cullingford, Tim E. "The Ketogenic Diet; Fatty Acids, Fatty Acid-Activated Receptors and Neurological Disorders." PLEFA 70 (2004): 253-264.
Fattorusso, Antonella, Lorenza Di Genova and Giovanni Battista Dell’Isola, et al. "Autism Spectrum Disorders and The Gut Microbiota." Nutr 11 (2019): 521.
Dong, N., Z. R. Li, P. Qin, C. and X. Qiang, J et al. "Risk Factors for Clostridioides Difficile Infection in Children: A Systematic Review and Meta-Analysis." JHI 130 (2022): 112-121.
Santocchi, Elisa, Letizia Guiducci and Francesca Fulceri et al."Gut to Brain Interaction in Autism Spectrum Disorders: A Randomized Controlled Trial on The Role of Probiotics on Clinical, Biochemical and Neurophysiological Parameters." BMC psychiatry 16 (2016): 1-16.
Santocchi, Elisa, Letizia Guiducci and Margherita Prosperi, et al. "Effects of Probiotic Supplementation on Gastrointestinal, Sensory and Core Symptoms in Autism Spectrum Disorders: A Randomized Controlled Trial." Front Psychiatry 11 (2020): 550593.
Chadman, Kathryn K. "Making Progress in Autism Drug Discovery." Expert Opin Drug Discov 9 (2014): 1389-1391.
Settivari, Ashrith and Kamala K. Maddali. "A Review on Promising Genetic Biomarkers and Therapeutic Interventions for Advancing Precision Medicine Principles for Autism." Future Medicine AI 1 (2023): FMAI7.
Koch, Elise and Ditte Demontis. "Drug Repurposing Candidates to Treat Core Symptoms in Autism Spectrum Disorder." Front pharmacol 13 (2022): 995439.