Tatsiana Astapovich1*, Yaron Goikhman2
1Obstetrician‑Gynecologist, Israeli Medical Center for Reproduction and Family Health, Tashkent, Republic of Uzbekistan
2MD, MSc, Israeli Medical Center for Reproductive Medicine and Family Health, Uzbekistan, ORCID: 0009-0006-7996-6351
*Correspondence: Tatsiana Astapovich, Obstetrician‑Gynecologist, Israeli Medical Center for Reproduction and Family Health, Tashkent, Republic of Uzbekistan. E-mail: Dr.astapovich2005@gmail.com
Citation: Tatsiana Astapovich. “Gynecological Morbidity and the Organization of Effective Prevention and Early Diagnosis Measures Among the Female Population of Central Asia.” J Gynecol Matern Health (2026): 127. DOI: 10.59462/3068-3696.4.1.127
Received date: 07 Jan, 2026; Accepted date: 24 Jan, 2026; Published date: 30 Jan, 2026
Copyright: © 2026 Tatsiana Astapovich. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Background: Diseases of the female reproductive system remain a significant public health challenge worldwide, particularly in regions with limited access to high-quality medical services. Gynecological morbidity is influenced by biological, social, cultural, and healthcare-system factors. In Central Asia, data on female reproductive health are limited, and late presentation often contributes to poorer outcomes.
Objective: To analyze the structure of gynecological morbidity among women seeking gynecological care in Tashkent, Uzbekistan, and to identify key factors influencing healthcare utilization, emphasizing prevention, early diagnosis, and targeted interventions for high-risk groups.
Materials and Methods: A retrospective analysis of 91 medical records of women attending gynecological consultations in 2024 at the Israeli Medical Center for Reproduction and Family Health was conducted. Patients’ age, reproductive history, parity, reasons for consultation, and diagnosed gynecological conditions were analyzed. Subgroup analyses were performed according to age, parity, and symptomatology. Descriptive statistics and chi-square tests were used to evaluate associations between parity, age, and cervical pathology.
Results: Cervical pathology constituted the largest proportion of gynecological morbidity. Chronic cervicitis was diagnosed in 45% of patients, cervical dysplasia grade I in 13.7%, and HPV-associated cervical pathology in 7%. Condylomatosis of vulva accounted for 15%, endometriosis 7%, MCD 6%, PID 6%, and fibroids 3%. High parity (≥3 births) was significantly associated with cervical pathology (p<0.05). Preventive visits represented only 13% of consultations, whereas 52% of women sought care due to symptoms.
Conclusions: Cervical diseases are the leading component of gynecological morbidity. Low preventive visit rates and delayed care-seeking highlight the need for enhanced screening, education, and targeted interventions, especially among multiparous women and those in remote regions. Strategies integrating telemedicine, outreach programs, and vaccination are recommended.
Keywords: Gynecological Morbidity, Cervical Pathology, HPV, Prevention, Early Diagnosis, Central Asia, Multiparity
Diseases of the female reproductive system remain a major contributor to morbidity and impaired quality of life among women worldwide. They encompass a broad spectrum of conditions, including cervical and endometrial pathology, ovarian disorders, menstrual dysfunction, and Sexually Transmitted Infections (STIs) [1,2]. Globally, cervical cancer accounts for approximately 600,000 new cases annually and remains a leading cause of cancer-related mortality in women, particularly in low- and middle-income countries [3,4].
In Central Asia, the burden of gynecological morbidity is compounded by socio-cultural, economic, and infrastructural factors. Many women have limited awareness of preventive care, and healthcare access is often unevenly distributed, with specialists concentrated in urban centers. Geographic barriers, including mountainous and desert regions, further restrict access to timely medical consultation [5,6]. These factors contribute to delayed presentation, underdiagnosis, and suboptimal treatment outcomes.
High parity is a recognized risk factor for cervical pathology and reproductive complications [7]. In Uzbekistan, total fertility rates remain relatively high (3.4 children per woman in 2023), and many women have limited access to routine gynecological surveillance [8]. Social barriers, cultural beliefs, and economic limitations also influence women’s healthcare-seeking behavior, often prioritizing acute or pregnancy-related concerns over preventive visits [6,9].
Although HPV vaccination was introduced nationally in 2019, studies suggest that coverage gaps and limited follow-up screening persist [10,11]. Consequently, understanding the structure of gynecological morbidity and factors influencing healthcare utilization is essential to develop targeted preventive strategies.
This study aims to evaluate the prevalence and structure of gynecological morbidity among women attending gynecological care in Tashkent, identify associations with age and parity, and provide evidence-based recommendations for prevention and early diagnosis in Central Asian settings.
This retrospective study analyzed medical records of 91 women aged 18–65 years who attended gynecological consultations at the Israeli Medical Center for Reproduction and Family Health, Tashkent, in 2024. Inclusion criteria were women seeking gynecological care for any reason, including preventive visits, infertility evaluation, or symptomatic complaints. Exclusion criteria included incomplete medical records or referral for non-gynecological conditions.
Data Collection
Data extracted included:
Age, age at menarche, parity
Reason for consultation (preventive, symptomatic, infertility, pregnancy-related)
Diagnosed gynecological conditions (cervical pathology, endometriosis, PID, MCD, fibroids, vulvar or vaginal lesions)
Ethical Considerations
The study protocol was approved by the Israeli Medical Center for Reproduction and Family Health. Patient confidentiality was maintained, and all data were de-identified prior to analysis.
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics. Categorical variables were expressed as frequencies and percentages. Chi-square tests assessed associations between parity, age, and cervical pathology, with significance set at p<0.05.
Patient Characteristics
Age ranged from 18 to 65 years.
Age at menarche ranged from 11–15 years (mean 12.7 ± 1.1).
High parity (≥3 births) was statistically significantly associated with cervical pathology.
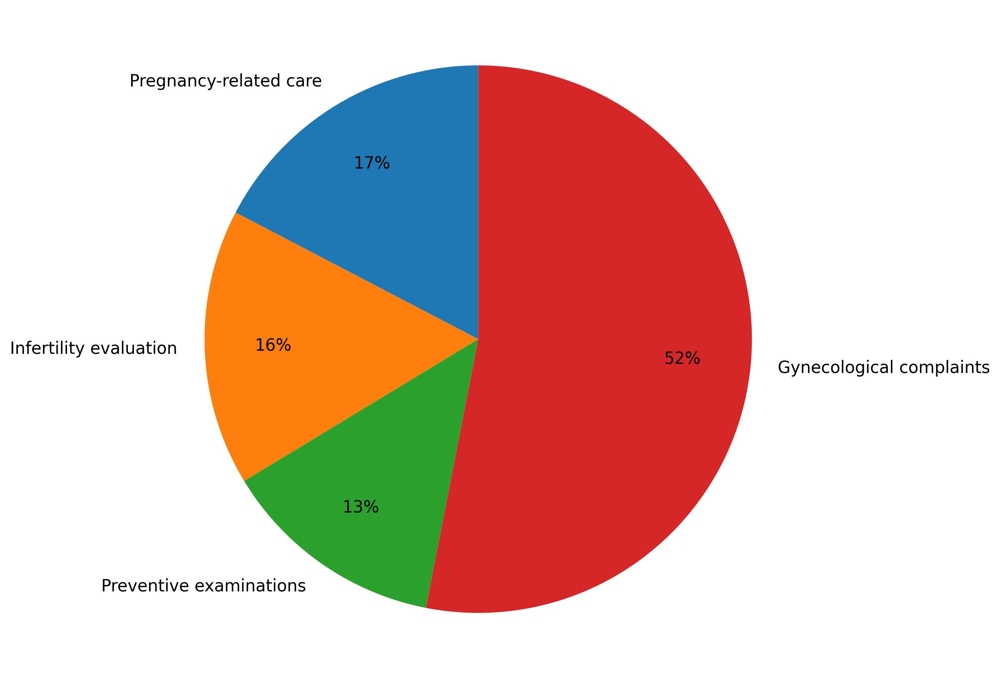
Figure 1: Distribution of consultation reasons (n=91)
17% attended for pregnancy-related care, 16% for infertility evaluation, 13% for preventive examinations, 52% for gynecological complaints.
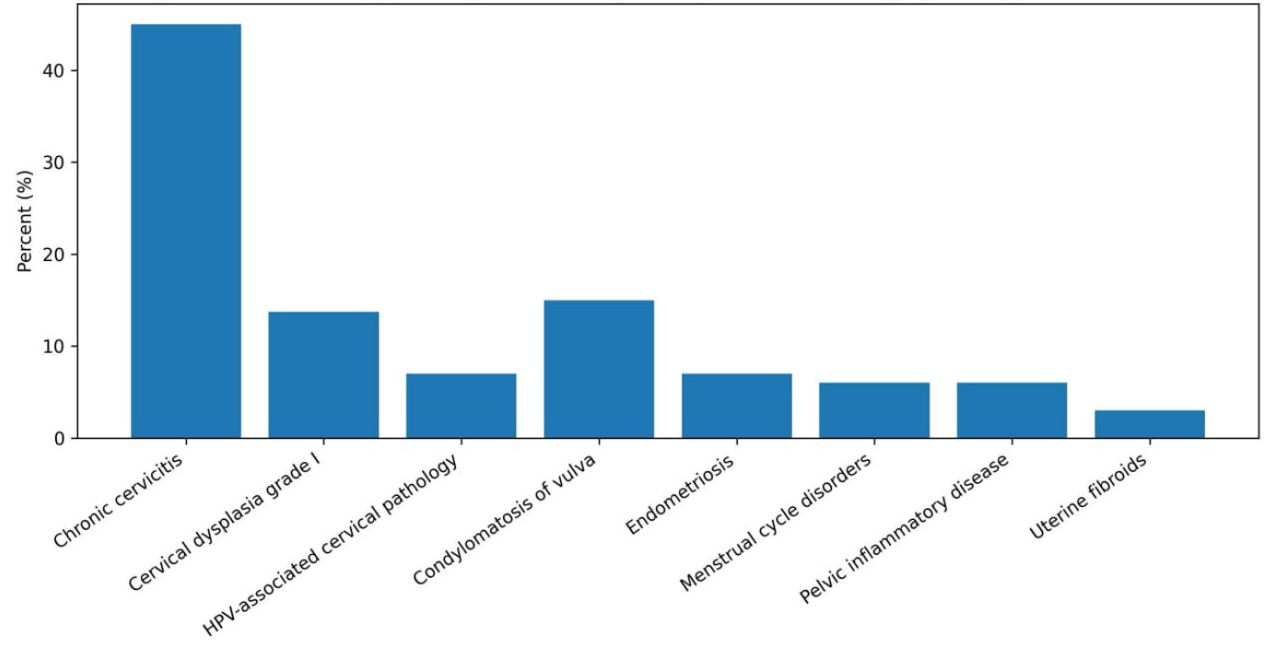
Figure 2: Structure of gynecological diagnoses by category
Table 1 summarizes the structure of gynecological diagnoses among the study population. The most prevalent condition was chronic cervicitis, diagnosed in 45% of patients. Condylomatosis of the vulva accounted for 15% of cases, while cervical dysplasia grade I was identified in 13.7%. HPV-associated cervical pathology was observed in 7% of women, as was endometriosis. Menstrual cycle disorders and pelvic inflammatory disease were each diagnosed in 6% of cases, and uterine fibroids were identified in 3% of patients.
|
Diagnosis |
% |
|
Chronic cervicitis |
45.0 |
|
Vulvar condylomatosis |
15.0 |
|
Cervical dysplasia I |
13.7 |
|
HPV-associated |
7.0 |
|
Endometriosis |
7.0 |
|
PID |
6.0 |
|
MCD |
6.0 |
|
Fibroids |
3.0 |
Table 1: Structure of gynecological diagnoses among the study population (n = 91)
High parity was significantly associated with cervical pathology (p=0.021).
Subgroup Analysis
Women attending for preventive visits had lower rates of cervical pathology compared to symptomatic women (8% vs 24%, p<0.05).
Condylomatosis predominantly affected women with recent onset of sexual activity (<1 year).
PID and MCD were often associated with concurrent infections or history of untreated gynecological complaints.
This structure is shown in Figure 2.
The predominance of cervical pathology in this population is consistent with global patterns and highlights the ongoing burden of HPV-associated diseases [2,5]. The significant association between high parity and cervical pathology underscores the need for targeted surveillance and preventive strategies for multiparous women.
Low rates of preventive visits (13%) indicate insufficient awareness and possible socio-cultural barriers to early gynecological evaluation. Most women seek care only after symptom development, reducing the effectiveness of screening programs [6,9].
Preventive measures, including regular cervical cytology, HPV testing, and vaccination, are critical. Uzbekistan achieved 94% first-dose HPV coverage among girls aged 12–14 by 2022 [7,8], but gaps in follow-up and adult vaccination remain.
Integration of telemedicine and mobile outreach clinics could address geographic and logistical barriers, particularly in remote areas. Evidence suggests that digital reminders, community education, and home-based sample collection can improve participation in screening programs [12–14].
Comparative data from other Central Asian countries indicate similar trends: high parity and limited preventive visits are associated with elevated cervical pathology and late-stage diagnoses [15].
Single-center design may limit generalizability; multicenter studies recommended.
Cervical pathology is the leading component of gynecological morbidity among women seeking care in Tashkent.
High parity (≥3 births) is a key risk factor, necessitating enhanced monitoring and preventive examinations.
Low preventive visit rates reflect delayed healthcare-seeking behaviour and inadequate awareness.
Strategic priorities include systematic screening, HPV vaccination, workforce distribution, telemedicine integration, and community education.
Special attention should be given to multiparous women and residents of remote regions.
Acknowledgments/Funding/Disclosures
The author thanks the staff of the Israeli Medical Center for Reproduction and Family Health for their support in data collection and patient management.
Conflict of Interest
The author declares no conflict of interest.
World Health Organization. Cervical cancer fact sheet. WHO; 2024. Available from: https://www.who.int/health-topics/cervical-cancer
Walboomers, Jan MM, Marcel V. Jacobs, M. Michele Manos, F. Xavier Bosch, J. Alain Kummer, Keerti V. Shah, Peter JF Snijders, Julian Peto, Chris JLM Meijer, and Nubia Muñoz. "Human papillomavirus is a necessary cause of invasive cervical cancer worldwide." The Journal of pathology 189, no. 1 (1999): 12-19.
Sung, Hyuna, Jacques Ferlay, Rebecca L. Siegel, Mathieu Laversanne, Isabelle Soerjomataram, Ahmedin Jemal, and Freddie Bray. "Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries." CA: a cancer journal for clinicians 71, no. 3 (2021): 209-249.
Bruni L, et al. Human papillomavirus and related diseases report: Uzbekistan. Vaccine. 2022;40(33):4749–4757.
Sharipova IP, Musabaev EI, Sadirova SS, et al. Prevalence of high-risk HPV genotypes among women in Uzbekistan, 2021–2023. J Gynecol Oncol. 2025;36(1):e7.
World Health Organization. Uzbekistan achieves high HPV vaccination coverage. WHO; 2022.
Ministry of Health, Uzbekistan. National Immunization Program Annual Report, 2022.
UNFPA Uzbekistan. HPV Testing and Cervical Cancer Screening Final Conference Report, 2022.
Toktanaliyeva AN, et al. Cervical cancer screening strategies in Central Asia. Int J Gynecol Obstet. 2023;161(1):10–19.
Brisson M, Bénard É, Drolet M, et al. Population-level impact of HPV vaccination: systematic review. Lancet Public Health. 2020;5(1):e34–e50.
IARC/HPV Centre. Human papillomavirus and related diseases report. 2023.
Khamidova A, et al. Digital interventions for cervical cancer screening in low-resource settings. Telemed J E Health. 2022;28(7):970–978.
Kovalenko M, et al. Mobile outreach clinics for reproductive health in Central Asia. BMC Womens Health. 2021;21:120.
World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. World Health Organization, 2020.
Zhang X, et al. Cervical cancer screening coverage and parity associations in Central Asia. Asian Pac J Cancer Prev. 2023;24(12):401–410.