Dr. Rohina Aggarwal1*, Dr Sumesh Choudhary2, Dr Kunur Shah3
1Professor and Head, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases & Research Centre (IKDRC), Ahmedabad, India
2Institute of Kidney Disease and Research Centre
3Institute of Kidney Disease and Research Centre, Ahmedabad
*Correspondence: Dr. Rohina Aggarwal, Professor and Head, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases & Research Centre (IKDRC), Institute of Transplantation Sciences (ITS), Ahmedabad, India, E-mail: drrohinaaggarwal@gmail.com
Citation: Rohina Aggarwal, Sumesh C, and Kunur S. “Imaging the Endometrium- Uterus Calcification Detection: Case Report.” J Gynecol Matern Health (2026): 130. DOI: 10.59462/3068-3696.4.2.130
Received date: 29 Jan, 2026; Accepted date: 13 Feb, 2026; Published date: 20 Feb, 2026
Copyright: © 2026 Rohina Aggarwal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Patients presenting with abnormal vaginal bleeding may show endometrial microcalcifications are loci of calcifications on ultrasonography. Usually associated with older age patient, postmenopausal state, atrophic endometrium, infertility and endometrial osseous metaplasia Tiny locules of gas and endometrial polyps may also present with hyperechoic areas. Calcification detected incidentally on ultrasonography may or may not indicate malignancy.
Age group of patients may be postmenopausal, reproductive or perimenopausal. Histopathological examination endometrial types may be atrophic, proliferative, benign endometrial polyps or endometrial malignancy. Microcalcifications can be concentric or amorphous, intraglandular or stromal or may be focally associated with minute papillary epithelial projections or degenerated endometrial glands. In reproductive age group common reasons of calcific endometritis are post-abortion (causing chronic inflammation from retained tissue after first and second trimester abortion), arteriovenous malformation, submucous fibroid, polyp and chronic endometritis (due to genital TB, non-specific chronic endometritis and pyometra). Final confirmation is by histopathology of biopsy specimens.
Biopsy results may show cell changes linked to hormone levels, or abnormal tissues, such as fibroids or polyps, uterine infections, such as endometritis and malignancy which result in abnormal bleeding.
We had come across one patient presented with postmenopausal bleeding and macrocalcification in the myometrium detected on ultrasonography.
Keywords: Endometrium, Endometrial Calcification, Postmenopausal Bleeding
Any significant deviation from a woman’s established menstrual pattern may be considered abnormal uterine bleeding and it depends on a woman's age, her menstrual history, and the use of medications such as hormonal pills. Premenopausal disorders that are well evaluated with ultrasound (US) include endometriosis, adenomyosis, and leiomyomas. In reproductive age group factors contributing to bleeding are ectopic pregnancy, placental factors including position, trauma, and infection, gestational trophoblastic disease, preterm labor, bone fragments and retained products of conception in pregnant patients while in nonpregnant patients especially in infertile women it is seen in patients with tubercular endometritis with Asherman Syndrome. While in the postmenopausal patient with abnormal uterine bleeding atrophic changes, hormone secreting tumours and carcinoma are important. Benign conditions should be distinguished from premalignant and malignant conditions Postmenopausal vaginal bleeding usually is caused by atrophic changes of the vagina or endometrium. Depending on age and risk factors, 1–14% of women with postmenopausal bleeding will have endometrial cancer.
Foreign bodies, trauma, polyps, infection and iatrogenic causes can be seen in all age groups. Commonest modality used for imaging and evaluation of the endometrium is pelvic ultrasonography either transabdominally or transvaginal.
Sometimes Hyster sonography and magnetic resonance imaging are used to evaluate abnormal endometrial thickness and abnormal appearance of the endometrium and uterine cavity.
Case 1
The present patient 52 years old, P2A1, postmenopausal for 3 years presented with postmenopausal bleeding single episode of painless vaginal bleeding with soakage of one pad. There was no history of dilatation & curettage, hormonal pill use or intra-uterine contraceptive device (IUCD) insertion.
Past menstrual history: was normal painless regular cycles at 26 days interval lasting for 4 to 5 days.
Past History: Use of unopposed estrogenic and medical comorbidities e.g. polycystic ovary syndrome, type 2 diabetes mellitus and chronic cough or tuberculosis were absent.
Family history: of gynecologic malignancy was not significant.
General Physical Examination: She was well built, well oriented to time, place and person and normal BMI. Her BP was 120/84 mm of Hg, PR was 88/minute. No pallor was detected. Systemic Examinations Cardiovascular System, Respiratory System were normal.
Per Abdomen: Examination was normal.
Per Speculum Examination: revealed atrophic vaginitis. No active bleeding through cervix or vagina or any abnormal vagina discharge was observed. No cervical polyp or fibroid was observed.
Per Vaginal Examination: revealed anteverted, small atrophic mobile uterus with clear fornices. Pap smear was taken.
Pap Smear: Cytological features consistent with reactive changes associated with acute inflammation. Negative for squamous intraepithelial lesion.
Transvaginal Sonography: Performed using Voluson E10 (GE Healthcare, Chicago, IL, USA) ultrasound machine endo-cavitary probe (3 to 8MHz). Longitudinal and transverse ultrasound images of uterus, endometrial lining and bilateral adnexa were obtained Uterus was 7.2 × 4.0 × 3.5 cm with a small intramural fibroid in the posterior fundal region. Endometrial thickness of 4mm with poor vascularity. In endometrium thick echogenic concentric line of calcification (Picture 1). Bilateral Ovaries were small and atrophic.
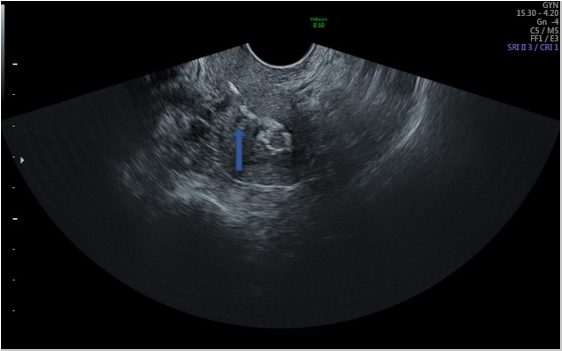
Picture 1: Uterus Showing Concentric Calcification The myometrium is heterogeneously echogenic in the fundus due to calcified arcuate arteries (asterisk)
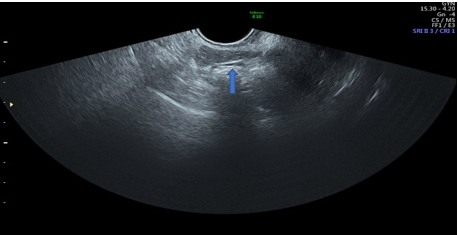
Picture 2: USG Showing Right Small Atrophic Ovary with No Antral Follicles
Picture 3: USG Showing Left Small Atrophic Ovary with No Antral Follicles

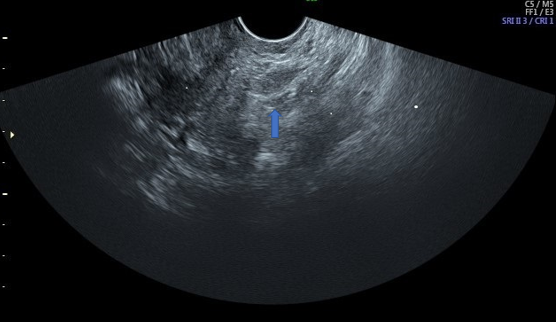
Picture 4: 3D USG Showing Echogenic Foci in the Centre of Uterine Cavity
Although there was no history of forgotten IUCD an X-Ray Pelvis was also done to detect forgotten IUCD, which revealed none (Picture 5).

Picture 5: X –Ray Pelvis Showing No Calcification in the Pelvic Region
Diagnostic hysteroscopy and guided biopsy was performed.
Office hysteroscopy was performed. There was slight difficulty in negotiating the internal os. Uterine cavity was normal with both ostia visible. Endometrium was slightly pale looking and atrophied otherwise normal looking. Using monopolar electrocautery and Glycine 1.5% as distending medium with a loop endometrial biopsy was taken and sent for histopathological examination in 10% formalin.

Picture 6: Hysteroscopy showing atrophied endometrium and normal uterine cavity
Histopathology Report: Inactive Endometrium with cystic atrophy, Myometrium unremarkable, No evidence of hyperplasia or malignancy.
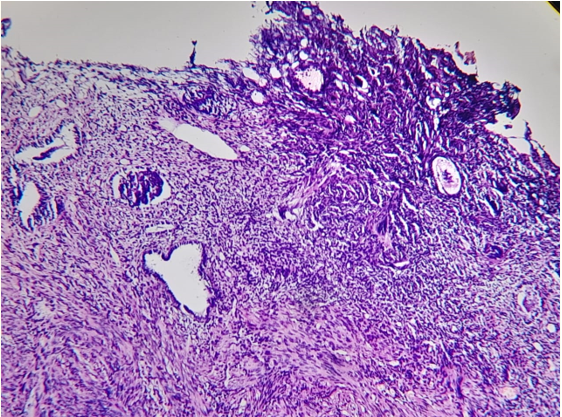
Picture 7: Picture showing atrophied endometrial gland-HE 50X
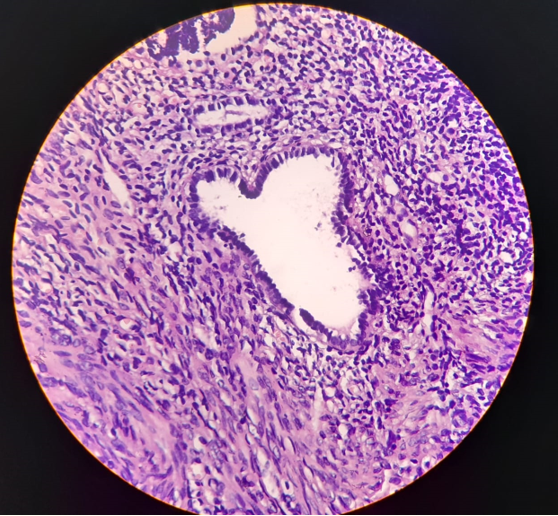
Picture 8: Picture showing atrophied endometrial gland - HE 200X
Vaginal bleeding is the presenting sign in more than 90% of postmenopausal women with endometrial carcinoma. The normal endometrium in a postmenopausal woman measures less than 5 mm. When there is fluid in the endometrial canal, the 2 layers of endometrium are measured separately and added together [1]. In a woman with postmenopausal bleeding, the endometrium is abnormal if it measures 5 mm or greater and this warrants endometrial biopsy [1,2]. In asymptomatic postmenopausal women without vaginal bleeding, the endometrium is abnormal if it measures 9 mm or greater, and this warrants endometrial biopsy [3]. Ultrasound signs that are more specific for endometrial cancer are a heterogeneous endometrium with colour flow or an indistinct endometrial-myometrium interface [1]. Cystic areas may be observed in cases of atrophic endometrium, hyperplasia, polyps, or cancer and the presence of cysts in the endometrium is nonspecific [4].
Some postmenopausal women are on hormone replacement and receive estrogen and progesterone that induces cyclical bleeding. It is important to measure their endometrium 4-5 days after the start of menses when it should measure less than 5 mm [1,2]. Menopause is defined as the absence of menses for greater than 12 months and typically occurs in women over 50 years of age [5].
Myometrium arterial calcifications are thought to increase with advancing age and may represent calcification of radial or arcuate arteries of the uterus.
They may have an increased association with atherosclerosis elsewhere. Arcuate arterial calcification manifests as symmetric, hyperechoic foci with acoustic shadowing at the periphery of the uterine myometrium. Both benign and malignant conditions affect the endometrium.
Endometrial ossification is an uncommon finding with several suggestions been made regarding the pathogenesis of this lesion [6] like osseous metaplasia from multipotential stromal cells, usually fibroblasts, which become osteo-blasts; continuous and strong endometrial estrogenic stimulation; retention of fetal bones that secondarily promote osteogenesis in the surrounding endometrium; implantation of embryonic parts without pre-existing bone after abortions at an early stage; dystrophic calcification of retained and necrotic tissues, usually after an abortion; chronic endometrial inflammation such as endometritis or pyometra; and metabolic disorders such as hypercalcemia, hypervitaminosis D or hyperphosphatemia [5]. The actual contribution of these pathogenic mechanisms is unknown.
The differential diagnosis of such unusual findings on ultrasound examination includes intrauterine contraceptive devices, foreign bodies, calcified submucous fibroids, endometrial tuberculosis, Asherman’s syndrome, and rarities such as heterotopic bone and uterine malignant mixed Mullerian tumour [2]. In premenopausal women, endometrial polyps may cause intermenstrual bleeding or menorrhagia [6]. In postmenopausal women, they may cause postmenopausal bleeding. The prevalence of malignancy ranges from 0.8%-8% and is greater in women over 60 years of age with vaginal bleeding. In a study by Costa-Paiva et al [7], the prevalence rate of malignancy in endometrial polyps in patients with postmenopausal bleeding was 4.5% compared to 1.5% in asymptomatic women. Other risk factors for malignant or premalignant polyps include obesity, chronic hypertension, chronic diabetes, and size greater than 15 mm [7] Some polyps have cystic areas that may be due to dilated glands [5].
In some cases, the endometrium cannot be evaluated with ultrasound that may be due to fibroids, the position of the uterus or endometrial cancer [2]. These patients benefit from further evaluation with MRI [8]. An axial uterus, obesity, coexisting myomas, adenomyosis, or previous uterine surgery can contribute to difficulty in obtaining reliable transvaginal ultrasound assessment of endometrial thickness and texture [9].
If blind sampling does not reveal endometrial hyperplasia or malignancy, hysteroscopy remains the gold standard for diagnosis of endometrial pathology [2] along with dilation and curettage in the evaluation of women with persistent or recurrent bleeding [10]. As rare cases of endometrial carcinoma (particularly type II) can present with an endometrial thickness of less than 3 mm, persistent or recurrent uterine bleeding should prompt a histologic evaluation of the endometrium regardless of endometrial thickness [10].
The most frequently used diagnostic methods were ultrasound (88.5% of articles) and hysteroscopy (85.7%) [11].
Submucosal fibroids may be differentiated from polyps with Hyster sonography as they are covered with normal endometrium and polyps are the protrusions in the endometrial cavity [6,12].
Endometrial polyps are localized overgrowths of endometrial glands and stroma with a vascular core [13]. They are most commonly seen in women who are at or near menopause [5,6]. The majority of polyps are asymptomatic [4] without risk factors for malignancy and can be managed conservatively. The treatment for symptomatic polyps is hysteroscopic excision [5,12].
Tamoxifen is given in some cases of early stage breast cancer to reduce recurrence and mortality. It is an estrogen antagonist in the breast but an estrogen agonist in the uterus where it induces endometrial proliferation with appear thickened with the “hyperechoic line sign” representing normal endometrium circumscribing the polyp [14]. Cystic areas may be observed in the thickened endometrium and sub endometrium [12]. Patients on tamoxifen with vaginal bleeding require biopsy when the endometrium measures 5 mm or greater. There is no consensus on how to manage asymptomatic patients on tamoxifen. Patients typically have annual screening pelvic ultrasonography.
On transvaginal ultrasound, the endometrium may retain products of conception (RPOC) may occur in women following spontaneous or therapeutic abortion or in the post-partum period (first 6 weeks post-delivery). Clinically, women will have vaginal bleeding or a discharge and a positive human chorionic gonadotropin. On ultrasound, the most specific sign for RPOC is an endometrial mass that may or may not demonstrate vascularity with colour flow. In at-risk women, the diagnosis may be made if the endometrium measures 10 mm or greater even without a focal mass or colour flow with a sensitivity of over 80% [15,16]. Conversely, the diagnosis of RPOC may be ruled out if the endometrium measures less than 10 mm without vascularity with a negative predictive value of 63%-80% [15,16]. The treatment options for RPOC are conservative management, prostaglandin E1 analogs and dilatation and curette (D&C) [16].
Go Another cause for vaginal bleeding in women following D&C is a post procedure arteriovenous malformation (AVM)). On greyscale US, uterine AVMs demonstrate heterogeneous echogenicity in the myometrium with cyst-like spaces creating a “spongy texture” due to hypoechoic tubular areas representing abnormal vascular channels. On spectral Doppler, they demonstrate marked hypervascularity with high-velocity, low-resistance arterial flow and abundant venous flow. The peak systolic velocities are typically in the 35-97 cm/second range but may be higher and the resistive index is in the 0.3-0.52 range (mean, 0.42) [17]. Spectral analysis of the normal uterine arteries reveals flows ranging from 9-44 cm/seconds and resistive indices ranging from 0.59-0.86 (mean, 0.73) [18]. There are also prominent parametrial vessels. Small AVMs may resolve spontaneously without intervention. However, when patients present with menorrhagia and anemia, angioembolization or hysteroscopy guided coagulation of spiral arteries may be required. It is important to make the diagnosis of AVM because D&C can lead to serious hemorrhage [6,18].
Another cause for hypervascularity in the myometrium in the post-partum period unrelated to D&C is enhanced myometrial vascularity from subinvolution of the placental implantation site. Like AVM's, subinvolution of the placental implantation site may cause vaginal bleeding that may resolve on its own or require embolization particularly when very high velocity flow is detected [16]. Uterine arteriovenous malformations may also be seen with gestational trophoblastic disease and in cases where the beta human chorionic gonadotropin is positive and high, it is important to consider placental site trophoblastic tumour that is a rare condition that may occur 4-36 months following pregnancy [18,19].
Endometrial abnormalities are seen in women of all age groups which can be easily evaluated using first-line imaging modality ultrasonography which is non-invasive, cheap cost effective and easily available tool for an initial evaluation of abnormal bleeding. No special preparation is needed and as an OPD procedure can be performed. It has high sensitivity and specificity for endometrial pathology detection. Furthermore, it guides us when to take endometrial biopsy to differentiate benign from premalignant or malignant conditions and their further management. Moreover, many benign conditions can be managed with imaging surveillance.The first pregnant woman had cirrhosis secondary to AIH, and she delivered by aesarean section. The patient had severe thrombocytopenia at the time of hospitalization. Unfortunately, she died due to massive thromboembolism at the 24th hour after delivery. The other patient had three recurrent abortions with a diagnosis of AIH. Low-dose low molecular weight heparin and low-dose acetylsalicylic acid along with low-dose prednisolone were administered during the course of the following pregnancies. The following pregnancies ended up with a living child.There is a high morbidity and mortality risk for both fetus and mother. Hepatic performance of the patients, thrombotic events, inflammatory disorders and autoimmune system activation must be the main concerns together with necessary precautions.
Nalaboff, Kenneth M., John S. Pellerito, and Eran Ben-Levi. "Imaging the endometrium: disease and normal variants." Radiographics 21, no. 6 (2001): 1409-1424.
Goldstein, Ruth B., Robert L. Bree, Carol B. Benson, Beryl R. Benacerraf, Jeffrey D. Bloss, Ruth Carlos, Arthur C. Fleischer et al. "Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound‐Sponsored Consensus Conference statement." Journal of Ultrasound in Medicine 20, no. 10 (2001): 1025-1036.
Smith‐Bindman, R., E. Weiss, and V. Feldstein. "How thick is too thick? When endometrial thickness should prompt biopsy in postmenopausal women without vaginal bleeding." Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology 24, no. 5 (2004): 558-565.
Atri, Mostafa, Soheyla Nazarnia, Ann E. Aldis, Caroline Reinhold, Patrice M. Bret, and George Kintzen. "Transvaginal US appearance of endometrial abnormalities." Radiographics 14, no. 3 (1994): 483-492.
Scoutt, Leslie M., Ulrike M. Hamper, and Teresita L. Angtuaco, eds. Ultrasound. OXFORD University Press, 2016.
Wilson, Stephanie R., C. E. Withers, S. R. Wilson, and W. R. Charboneau. "Diagnostic ultrasound." Philadephia: Elsevier Mosby Publisher 853 (2005): 863.
Costa-Paiva, Lucia, Carlos E. Godoy Jr, Armando Antunes Jr, Joyce D. Caseiro, Michael Arthuso, and Aarao M. Pinto-Neto. "Risk of malignancy in endometrial polyps in premenopausal and postmenopausal women according to clinicopathologic characteristics." Menopause 18, no. 12 (2011): 1278-1282.
O'Connell, Lawrence P., Melissa H. Fries, Ernest Zeringue, and Walter Brehm. "Triage of abnormal postmenopausal bleeding: a comparison of endometrial biopsy and transvaginal sonohysterography versus fractional curettage with hysteroscopy." American journal of obstetrics and gynecology 178, no. 5 (1998): 956-961.
Miller, Janet C., Isaac Schiff, James H. Thrall, and Susanna I. Lee. "Ultrasound and sonohysterography in the evaluation of abnormal vaginal bleeding." Journal of the American College of Radiology 5, no. 11 (2008): 1154-1156.
Cramer, Daniel W. "The epidemiology of endometrial and ovarian cancer." Hematology/oncology clinics of North America 26, no. 1 (2011): 1.
Sala, Evis, Suzanne Wakely, Emma Senior, and David Lomas. "MRI of malignant neoplasms of the uterine corpus and cervix." American Journal of Roentgenology 188, no. 6 (2007): 1577-1587.
Shi, Ann A., and Susanna I. Lee. "Algorithmic workup of abnormal vaginal bleeding with endovaginal sonography and sonohysterography: self-assessment module." American Journal of Roentgenology 191, no. 6_supplement (2008): S74-S78.
Jorizzo, Johanna R., Michael YM Chen, Deena Martin, Raymond B. Dyer, and Therese M. Weber. "Spectrum of endometrial hyperplasia and its mimics on saline hysterosonography." American Journal of Roentgenology 179, no. 2 (2002): 385-389.
Baldwin, Matthew T., Kika M. Dudiak, Brian Gorman, and Catherine A. Marks. "Focal intracavitary masses recognized with the hyperechoic line sign at endovaginal US and characterized with hysterosonography." Radiographics 19, no. 4 (1999): 927-935.
Durfee, Sara M., Mary C. Frates, Angela Luong, and Carol B. Benson. "The sonographic and color Doppler features of retained products of conception." Journal of ultrasound in medicine 24, no. 9 (2005): 1181-1186.
Sellmyer, Mark A., Terry S. Desser, Katherine E. Maturen, R. Brooke Jeffrey Jr, and Aya Kamaya. "Physiologic, histologic, and imaging features of retained products of conception." Radiographics 33, no. 3 (2013): 781-796.
Peitsidis, Panagiotis, Emmanouil Manolakos, Vasiliki Tsekoura, Rolf Kreienberg, and Lukas Schwentner. "Uterine arteriovenous malformations induced after diagnostic curettage: a systematic review." Archives of gynecology and obstetrics 284, no. 5 (2011): 1137-1151.
Huang, Madeline W., Derek Muradali, W. A. Thurston, Peter N. Burns, and Stephanie R. Wilson. "Uterine arteriovenous malformations: gray-scale and Doppler US features with MR imaging correlation." Radiology 206, no. 1 (1998): 115-123.
Zhou, Y., H. Lu, C. Yu, Q. Tian, and W. Lu. "Sonographic characteristics of placental site trophoblastic tumor." Ultrasound in Obstetrics & Gynecology 41, no. 6 (2013): 679-684.