Kingsley Agholor1,2*, Aimiehinor Edward Akhator3,4, Pudigha James Opomu2, Chichi Ukoha5, Chukwunonso Isaiah Enechukwu6, George Uchenna Eleje6,7, Ahizechukwu Chigoziem Eke8
1Coastal Specialist Clinic and Fertility Centre. Warri, Nigeria
2Department of Obstetrics and Gynaecology, Central Hospital, Warri, Nigeria
3Department of Obstetrics and Gynaecology, Delta State University Teaching Hospital, Oghara, Nigeria
4Department of Obstetrics and Gynaecology, Faculty of Clinical Science, Delta State University, Abraka, Nigeria
5Department of Obstetrics and Gynaecology, Barts Health NHS Foundation Trust, London, UK
6Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University Teaching Hospital Nnewi, Nigeria.
7Effective Care Research Unit, Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University, Awka, Nigeria.
8Division of Maternal Fetal Medicine, Department of Gynecology and Obstetrics, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA
*Correspondence: Kingsley Agholor, Coastal Specialist Clinic and Fertility Centre, Central Hospital Warri. Warri, Nigeria. Email: knagholor@yahoo.com
Received: 28 Oct, 2025; Accepted: 11 Nov, 2025; Published: 28 Nov, 2025.
Citation: Agholor K, Akhator AE, and Pudigha JO et al. “Laparoscopic retrieval of a partially extruded intrauterine contraceptive device following uterine perforation.” J Gynecol Matern Health (2025): 120. DOI: 10.59462/3068-3696.3.1.120
Copyright: : © 2025 Kingsley Agholor. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Uterine perforation and extrauterine migration of an intrauterine contraceptive device (IUCD) are uncommon but potentially serious complications.
Case Presentation: We report a 25-year-old para 1 Nigerian woman who developed persistent lower abdominal pain shortly after postpartum IUCD insertion. Imaging studies (abdominal x-ray and 3D-transvaginal scan) revealed an empty uterine cavity with the IUCD partially extruded into the peritoneal cavity. Laparoscopic exploration confirmed uterine perforation with blood tracking from the fundus. The device was successfully retrieved laparoscopically, and the patient recovered without complications.
Conclusion: Uterine perforation is a rare but serious complication of postpartum IUCD insertion. Early recognition, appropriate imaging, and timely referral to facilities with laparoscopic expertise are critical for optimal outcomes. Ensuring careful patient selection and skilled insertion practices may help reduce the risk of such complications and enhance the effectiveness of laparoscopic retrieval.
Keywords: Complications, Laparoscopic retrieval, missing IUCD, Uterine perforation.
Introduction
Intrauterine contraceptive devices (IUCDs) are wide ly used, cost-effective, and highly reliable long-acting reversible contraceptives [1]. It was first introduced by Richter in 1909 and later refined by Grafenberg in 1929 [2], IUCDs have since evolved into two ma jor categories: the copper-bearing intrauterine device and the levonorgestrel-releasing intrauterine system [3-5].
Although IUCDs are generally safe, complications may occur, including expulsion, malposition, infec tion, and pregnancy [3-5]. Uterine perforation, though rare, reported in approximately 0.4 to 1.6 per 1,000 insertions, remains the most serious complication,often occurring at the time of insertion [6]. Perfora tion may lead to extrauterine migration of the device, necessitating radiological evaluation and, in many cases, laparoscopic removal.
Existing literature reports a spectrum of perforation presentations, ranging from asymptomatic cases to severe abdominal pain or organ involvement. Most cases describe complete intraperitoneal migration. However, partial extrusion of an IUCD, with one segment embedded within the myometrium and another within the peritoneal cavity, remains relatively un common.
The novelty of this case lies in the presentation of a partially extruded IUCD diagnosed using sequential 2D and 3D transvaginal ultrasonography and subse quently retrieved laparoscopically, demonstrating the importance of advanced imaging and minimally in vasive expertise in low-resource settings. We present a case of postpartum uterine perforation with partial IUCD extrusion in the Niger Delta region of Nigeria, highlighting the diagnostic value of 3D ultrasonog raphy and the effectiveness of laparoscopic retrieval.
Case Presentation
Patient information
A 25-year-old Nigerian woman, para 1, presented to our tertiary centre with a three-week history of persis tent lower abdominal pain. She had delivered vagin ally eight weeks earlier without complications. Her postpartum recovery had been uneventful until the insertion of an IUCD at a private healthcare facility. The specific type of IUCD inserted was not docu mented. The device had been placed approximately five weeks postpartum.
Clinical findings
The patient reported that the abdominal pain com menced within hours of insertion. The pain was dull, constant, and localised to the lower abdomen, without radiation. She denied fever, heavy bleeding, vaginal discharge, gastrointestinal disturbances, or urinary symptoms. No difficulty during insertion had been recorded in the referring facility.
On examination, she was haemodynamically stable. Abdominal assessment revealed generalised lower abdominal tenderness without guarding or rebound, and there were no clinical signs suggestive of peritonitis.
Diagnostic assessment
A plain abdominal radiograph demonstrated an IUCD positioned abnormally within the pelvis (Figure 1). Two-dimensional transvaginal ultrasonography re vealed a hyperechogenic focus near the uterine fun dus, raising suspicion of uterine perforation (Figure 2). Three-dimensional transvaginal imaging offered superior anatomical detail, clearly demonstrating: an empty uterine cavity, partial extrusion of the IUCD through the posterior lower uterine segment into the peritoneal cavity, and a hyperechogenic spot corres ponding to fundal trauma, likely resulting from a prior unsuccessful blind retrieval attempt (Figures 3–8). These findings confirmed uterine perforation with partial migration of the device.

Figure 1. Plain abdominal x-rays showing IUCD.
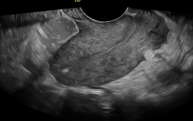
Figure 2. Shows a hyperechogenic area at the fundus that indi cated the area of perforation during the blind dilatation and curet tage that she underwent before presentation to our facility.
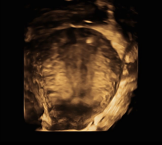
Figure 3. This shows the area of perforation at the fundus on 3D

Figure 4. Shows the site of fundal perforation with uterine sound

Figure 5. Shows 3D image of IUD at the lower uterine segment with evidence of perforation
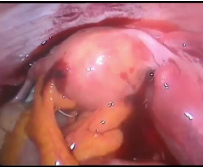
Figure 6. Shows the area of fundal perforation and hemoperito neum.

Figure 7. Shows the IUCD at the lower uterine segment partly extruded into the peritoneal cavity with hemoperitoneum.
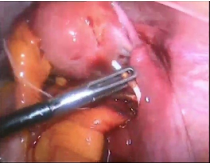
Figure 8. Shows IUCD being removed during laparoscopic surgery with a grasper
Therapeutic intervention
After detailed counselling, the patient consented to laparoscopic retrieval. At laparoscopy, a panoramic view revealed blood oozing from the uterine fundus with a collection in the recto-uterine space. The IUCD was visualised at the previously identified site, with one arm extruding into the peritoneal cavity. Using an atraumatic grasper, the device was gently mobilised and removed via the umbilical port without difficulty. The procedure was completed without intraoperative complications.
Follow-up and outcomes
The patient’s postoperative recovery was uneventful. She was discharged on postoperative day one, fol lowing clinical improvement and adequate pain con trol. At her two-week follow-up, she remained asymp tomatic, with complete resolution of abdominal pain. She received detailed contraceptive counselling, and alternative methods were discussed and offered.
Discussion
Uterine perforation is an uncommon but serious complication of intrauterine contraceptive device (IUCD) insertion, with an incidence estimated at ap proximately 2 per 1,000 insertions [1,7]. It is regarded as the most severe insertion-related complication and typically occurs during uterine sounding or IUCD placement, often due to inadequate assessment of uterine position or orientation prior to insertion [2-5]. Evidence suggests that the risk is further increased during the immediate puerperal period, during breastfeeding, with certain IUCD types, and when insert ed by less-experienced providers [3,6,8] Perforation may be classified as primary, occurring at the time of insertion, as in this case, or secondary, where migra tion occurs weeks or months after insertion [1].
Perforations may be either complete or partial. Com plete perforation occurs when the device breaches all three uterine layers, endometrium, myometrium, and serosa, and is found freely within the peritoneal cav ity. In contrast, partial perforation refers to embed ment within the myometrium without complete pas sage of the device [2]. The present case represents partial perforation, as a portion of the IUCD remained embedded within the myometrium despite a 12-hour interval between diagnosis and operative retrieval. Clinical presentation varies considerably. Many pa tients experience acute lower abdominal pain im mediately after insertion, as in this case. Others may present with abnormal vaginal bleeding, bowel or bladder injury, haemoperitoneum, haematoma for mation, abscess, adhesions, or peritonitis [1,5-8]. Importantly, up to one-third of perforations may be asymptomatic, leading to delayed recognition [9,10]. This highlights the importance of careful post-inser tion counselling and early evaluation of persistent pain.Ultrasound, particularly transvaginal ultrasonography, is the first-line imaging modality for suspected per foration as it is accurate, cost-effective, and readily available [2,5, 7-9]. In this patient, three-dimensional transvaginal ultrasound clearly delineated the loca tion and depth of IUCD embedment, enabling precise surgical planning. Plain abdominal radiography, CT, and MRI are alternative imaging options; although more expensive and less accessible in many low-re source settings, CT and MRI can be particularly use ful for defining extra-uterine migration and associated complications [7,9].
Management strategies depend on the degree of perforation, symptom severity, and device loca tion. Hysteroscopic removal is recommended when the IUCD is only superficially embedded within the endometrium or myometrium [6,11,12]. However, for partially or completely perforated devices extending beyond the uterine wall, surgical retrieval is indicat ed. Laparoscopy is widely regarded as the preferred minimally invasive approach due to superior visual isation, reduced blood loss, shorter recovery times, and fewer postoperative complications when compared to laparotomy [6,11]. Recent reports demon strate high success rates with laparoscopic retriev al even in complex cases involving adjacent organ involvement [12]. In order to avoid this potential life threatening complications of IUCD during insertion, it is paramount to know the orientation and shape of the uterus, proper traction, stabilization and to have a trained or skilled personnel perform the procedure of IUCD insertion [1].
In the present case, laparoscopy provided excellent visualisation of the perforation site and facilitated safe removal of the IUCD. The intraoperative finding of blood within the recto-uterine pouch corresponded with the perforation at the uterine fundus visualised on ultrasound. While laparotomy remains an option, particularly in unstable patients, cases with significant haemoperitoneum, or when laparoscopic expertise is unavailable, current recommendations from the Fac ulty of Sexual and Reproductive Healthcare (FSRH) guidance favour laparoscopic retrieval of IUCD or management whenever feasible [13,14].
Possible short-term complications of perforation and retrieval include haemorrhage, infection, bowel or bladder injury, and postoperative adhesions [1,4]. Long-term sequelae may include chronic pelvic pain, subfertility, or recurrent adhesions, although these outcomes are uncommon when timely surgical management is provided [10]. Laparoscopic techniques are associated with better long-term recov ery and reduced adhesion formation compared with open surgery [12].
This case reinforces several important considera tions for family planning practice. Postpartum IUCD insertion carries an increased risk of perforation due to uterine enlargement, softening, and involutional changes. Persistent abdominal pain after insertion should raise prompt suspicion of perforation, war ranting immediate imaging. Three-dimensional trans vaginal ultrasonography, as demonstrated here, is invaluable for localising misplaced devices. Early re ferral to centres with laparoscopic capability is essen tial to minimise morbidity. In addition, follow-up visits after IUCD insertion are important to assess and con firm that the device has been correctly positioned.
Conclusion
Uterine perforation is a rare but clinically significant complication of postpartum IUCD insertion. Early recognition, appropriate imaging, and timely referral to facilities with laparoscopic expertise are critical for optimal outcomes. Adhering to FSRH guidance on careful patient selection, uterine assessment prior to insertion, and ensuring skilled, well-trained practitioners perform insertions can further reduce the risk of such complications.
Acknowledgements
The authors express their gratitude to the index patient for her informed consent to participate in this presentation (signed consent was obtained from her).
Disclosure
The authors declare that there is no conflict of interest in this work.
Ethical Consideration
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
No specific funding was received from funding agencies in the public, commercial or not-for-profit sectors.
Author Contributions
KA, and AEA conceived, supervised the study and performed the surgery; GUE, PJO, CU and CIE ana lyzed data; KA, AEA, GUE, PJO, CU, ACE and CIE made manuscript revisions. All authors reviewed the results and approved of the final version of the manuscript.
Ethics Approval and Consent to Participate
Not applicable
Consent for Publication
Written informed consent was obtained from the patient for publication of her de-identified data and images.
Availability of Data and Materials
Data sharing is not applicable to this article as no datasets were generated or analysed during this study.
References