Amitabh Mitra1*, Yetish Ramsurrup2
Head of Emergency Medicine and Gender Based Violence, Cecilia Makiwane Hospital, Mdantsane, Eastern Cape, South Africa.
Medical doctor, Emergency Medicine Department, Dora Nginza hospital, Port Elizabeth, Eastern Cape, South Africa.
Received: 28 March 2024; Accepted: 09 April 2024; Published: 12 April 2024
Citation: Mitra, Amitabh, and Yetish Ramsurrup. “Literature Review in Crush Syndrome.” J Fam Med Clin Res (2024): 102. DOI: 10.59462/JFMCR.1.1.102.
Copyright: © 2024 Mitra A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Crush Syndrome is also known as Traumatic Rhabdomyolysis and is referred as Bywater’s Syndrome. It is a group of symptoms that finally leads to severe shock and renal failure. This syndrome seems to have its origins from the second World War, especially during the bombing of London when the British Physician Eric Bywaters described it in detail in a number of patients who were crushed due to a building collapse. In this historical article first published in the British Medical Journal, March 1941 issue, Dr. Bywaters explains the symptoms of small urinary output, thirst, generalised edema and incessant vomiting. The blood urea and potassium becomes progressively higher. Death occurs suddenly and frequently within a week. Necropsy reveals necrosis of muscles and in the renal tubules, degenerative changes and casts containing brown pigment. [1]
Where it develops
Any area of the body which is trapped for more than four hours and arterial blood flow is compromised. Freeing the limb or other body parts from entrapment not only results in release of by-products of metabolism and tissue destruction but also involves the potential for cardiac arrest. In prolonged entrapment, ‘Smiling death’ may occur if providers do not take proactive measures. [2]
Muscle breakdown products in the form of Myoglobin, Potassium and Phosphorus is released into the blood. The renal toxicity is due to Myoglobin. Life threatening dysrhythmias may also develop from increased Blood Potassium levels. Hyperphosphatemia can lead to calcifications that can interfere with normal blood flow and normal nervous tissue function. Increased levels of Uric Acid, Lactic Acid and Potassium may also cause Metabolic Acidosis.
Wide spectrum of traumatic rhabdomyolysis in earthquake victims. The Iran earthquake experience
In present study the authors evaluate victims of Bam earthquake to show different stage of muscle trauma, from minor trauma with almost normal level of muscle enzyme to those with moderate trauma leading to crush injury and finally to advanced crush syndrome. Questionnaire consisted of clinical, biochemical and demographic items was designed and completed by our research team retrospectively. The authors divided the patients to crush and non-crush and also crush injury and crush syndrome, and then compared aforementioned items between them. The schematic algorithm of medical managements for decreasing of morbidity and mortality of earthquake’s victims -
All of earthquake victims
Step1: Crush injured
Step2: Crush syndrome
Step3: Death
For decreasing morbidity and mortality of these victims the main attention of rescue team should be prevention of crush syndrome and its consequences such as Compartment Syndrome and AKI. The authors have schematized in figure, this prevention can be done in 3 steps:
Step 1. Extrication of these patients and urgent initiation of early hydration therapy, while checking the most essential clinical and paraclinical factors such as; muscle enzymes, Bun, Creatinine, electrolytes and urine analysis
Step 2. Assessment the level of muscular trauma and utilization of appropriate management strategies accordingly, using high dose prophylactic hydration therapy (more than 10 liters/day) only in those whom are at risk of AKI and dialysis. The majority of victims (80%) with minor trauma and mild rhabdomyolysis do not need such enormous volumes of fluid. Through this kind of triage, we would be able to prioritized our treatment to the most severe and needed patients which would finally decrease morbidity and mortality of these patients. The authors unpublished data in Bam earthquake is strongly in favour of this policy.
Step 3. Fasciotomy or amputation, initiation of dialysis, ventilator support and ICU care if indicated to reduce mortality. [3]
The effect of ischemia reperfusion injury on skeletal muscle
Ischemia reperfusion (IR) injury occurs when tissue is reperfused following a period of ischemia, and results from acute inflammation involving various mechanisms. IR injury can occur following a range of circumstances, ranging from a seemingly minor condition to major trauma. (Figure 1) Hyperbaric (HBO) treatment can increase the partial pressure of oxygen in tissue. HBO treatment has been shown to be effective in reducing skeletal muscle IR injury in a rat tourniquet induced limb ischemia Hypothermia is commonly used to maintain amputated tissues prior to replantation.

Figure 1. Diagram showing cell injury can lead to free radical reactions in the surrounding area.
The use of local hypothermia during ischemia, during reperfusion, and during both was studied in a rat gracilis muscle flap model. Local hypothermia was shown to be protective when applied during the early reperfusion of skeletal muscle, suggesting a potential future clinical strategy for minimizing reperfusion induced IR injury. Some promising results have also recently been reported on the ability of low-level laser therapy to protect skeletal muscle against IR injury. [4]
Crush Syndrome in Africa
Crush syndrome may present after severe beatings, the most common presentation in Africa, not only as a result of entrapment
• Crush syndrome, when discovered early, can usually be managed conservatively and haemodialysis, a much more costly and high risk procedure, can be avoided.
• Emergency personnel must consider it in the differential diagnosis of victims of severe beatings with pigmenturia or tense compartments.
What’s new?
• Discusses the epidemiology of crush syndrome in a historical as well as present day, Africa-relevant context.
• Provides a thorough but simplified overview of the complicated pathophysiology of crush syndrome.
• Provides an approach to the management of crush victims at each stage of injury.
This review will discuss specifically rhabdomyolysis and AKI in the setting of crush injury with limb compression and ischaemia. With regard to outcomes from non-disaster settings but specifically trauma-related crush syndrome, 10–20% of patients develop renal dysfunction, with 1.5– 2% of patients requiring dialysis for oliguric renal failure. High-risk variables significantly associated with rates of renal impairment include delay to admission >12 h, severe metabolic acidosis with bicarbonate level less than 17, low initial haemoglobin, heavy pigmenturia, body surface area affected >18%, and high serum creatine kinase (CK) levels.
Diagnosis
Since aggressive early management of renal injury is essential in reducing morbidity and mortality associated with crush syndrome, having a high suspicion in the setting of significant trauma to the extremities or torso is necessary. Key components of the history include both duration and severity of the crush injury or assault, oral and intravenous fluid intake prior to arrival, and urine output. Signs of crush syndrome include frequently a painful and swollen extremity or other significant soft tissue injury with dark or red appearing urine, and poor urinary output. With regard to laboratory tests, the inexpensive urine dipstick showing blood, with absence of red blood cells on microscopic review is highly suggestive and specific for myoglobinuria and thus rhabdomyolysis. A serum CK level can be helpful, and serial levels as well as urine output should be monitored as levels over 8500 U/L have been correlated to acute renal failure and the need for dialysis, though how strong that correlation is appears to still vary between studies.
Management
Because the complications of crush syndrome are lifethreatening, the key to management is prevention. Whenever possible, aggressive fluid resuscitation should begin in all crush victims prior to their extrication.22 Studies have found that patients often remain hemodynamically stable while entrapped, but it is after extrication that hypotension and renal injury begins, secondary to the inflammatory cascade that is part of limb crushing and ischaemia-reperfusion discussed above. Intravenous fluids help to prevent renal ischaemia by increasing perfusion and force diuresis, with the goal to avoid myoglobin cast obstruction of the tubules, though its efficacy appears to fall after the first 6–12 h. It is important to keep in mind the role that high volume normal saline infusion may play in furthering metabolic acidosis- by diluting the serum bicarbonate as well as by contributing negative chloride ions, thus generating a hyperchloraemic metabolic acidosis. Should that arise, more bicarbonate may be added and less isotonic saline can be infused, via switching the base fluid to half normal saline (0.45% normal saline) if the pH trends towards significant acidosis.
• One litre of isotonic saline, alternating with 1 L half isotonic saline with 50 mEq sodium bicarbonate or
• Two litres of isotonic saline, followed by 1 L half isotonic saline with 50 mEq sodium bicarbonate.
For this reason, in addition to frequent monitoring of potassium levels, arterial pH should be followed and not exceed 7.5, and calcium and bicarbonate levels should guide continued therapy. Hypocalcaemia should be treated only if severe or if the patient is symptomatic, as deposited calcium in damaged muscles may mobilize later, resulting in hypercalcaemia. In patients with a minimal urine output >20 mL/h, addition of a 20% mannitol solution to each litre of fluid at a rate of 5 g/h can be considered to encourage an osmotic diuresis. If after a trial period urine output has not improved to 200 mL/h, mannitol should be discontinued. The benefit of mannitol is primarily theoretical and more randomized controlled trials need to be done to establish true clinical efficacy over hydration with normal saline alone. [5]
Crush recommendations: a step forward in disaster nephrology
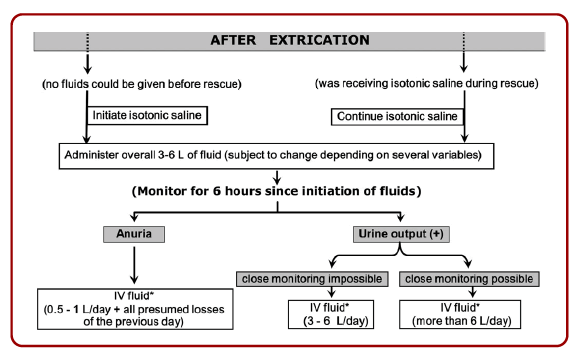
The Authors summarized nine prominent topics: fluid administration, hyperkalaemia, hypocalcaemia, acidosis, fasciotomy, amputation, dialysis, planning and logistic organization. Fluid resuscitation should be unequivocally started when the victim is still under the rubble or, if this appears impossible, during or immediately after extrication. The quantity to be administered depends on several factors. During extrication, a flow of 1L/h is recommended during the first 2 hours, then 0.5L/h. After extrication, if the patient did not yet receive fluid, 1L/h is recommended as starting dose as soon as possible while in total 3-6 L should be given over a period of 6 hours. The subsequent fluid administration depends on the urinary response. In case of sustained anuria after exclusion of hypovolaemia, the recommended volume is restricted to 500 – 1000 mL/ day plus the equivalent of all measured or estimated fluid losses of the previous day. (Figure 2)
Hyperkalaemia
Hyperkalaemia remains one of the main killers in crush especially by causing arrhythmia and cardiac standstill. Muscle devastation, causing massive release of intracellular contents into the blood stream, results in dramatic increases in serum potassium, which is further enhanced by acidosis and loss of kidney function in addition, hyperkalaemia is synergistic with hypocalcaemia, another frequent biochemical disturbance in crush (see below). Their negative inotropic and arrhythmogenic impact on the heart increase the risk of renal hypoperfusion and thus of AKI. To cope with hyperkalaemia, several preventive and therapeutic measures are recommended. Several therapeutic options act immediately (Ca Gluconate, b-agonists, bicarbonate, glucose-insulin); they are, however, not definitive, as most of them only cause a relocation from plasma to intracellular and/or are short acting.
Hypocalcaemia
Next to hyperkalaemia, the most important electrolyte disturbance is hypocalcaemia, resulting from the influx of calcium into the muscle due to functional impairment of the muscular cell membrane; it may result in paraesthesia, tetany, seizures, hypotension, bradycardia, impaired cardiac contractility and arrhythmia. The calcium accumulated in the muscles is released back into circulation at a later stage when the muscular lesions are healing, hence creating at that time a potential for hypercalcaemia. Therefore, in crush, correction of hypocalcaemia is recommended only if it is symptomatic.
Acidosis
Acidosis causes dysfunction of a host of organ systems and enhances hyperkalaemia. The recommendations advise correction only from a pH below 7.1 on since bicarbonate treatment can induce electrolyte disturbances by itself. In case of severe hyperkalaemia, alkalinisation of plasma may help in obtaining a quick decrease in serum potassium levels Dialysis is an option to correct acidosis without inducing unphysiologic shifts of other electrolytes. [6]
Continuous renal replacement therapy and blood transfusions in treating patients with crush syndrome
The early treatment of crush syndrome should involve supplementing blood volume, avoiding shock and restoring normal blood circulation and tissue perfusion as early as possible so as to protect the functions of important organs and relieve their injuries to the largest extent possible. A large amount of timely and effective fluid infusion dilatancy could increase the success rate of rescue. Coagulation disorders, massive capillary hemorrhage, bleeding on the wound surface and disputes about saving crushed limbs inevitably delay treatment and simultaneously increase the demand for blood transfusions.
Some reports indicate that if patients who suffered from massive hemorrhage had secondary low body temperature, acidosis, even DIC and other serious pathophysiological changes, then fluid infusion of large amounts of fluid and a decrease in the diluting coagulation ingredients might be just a secondary factor causing the abnormal coagulation [6-8]. Therefore, blood component transfusion was especially important. After the shock was stabilized, osteofascial compartment incision decompression should be performed to remove the necrotic tissue as early as possible; if necessary, amputation should also be carried out. For patients with acute renal failure, if treatment with an active dilatant or a large dose of furosemide was not effective, then dialysis should be performed in a timely manner.
Compartment Syndrome and its relation to Crush Syndrome
The term Compartment Syndrome is used to refer to local muscle ischemia and contracture resulting from Edema and increased pressure within the osteofascial compartment. Crush Syndrome refers to the systemic manifestations of muscle necrosis including myoglobinuric renal failure, shock and the cardiac sequelae of Acidosis and Hyperkalemia [8]. Although both are intimately related to each other yet one must recognise each of these entities separetely.
Crush Syndromes in Eastern Cape
Crush Syndromes commonly seen in township hospitals are related to interpersonal violence. Assaulting an individual by the community with fists, kicks, sticks and metal rods usually causes such a systemic disorder. Sjambok Injuries due to assault by sticks or metal rods causes red parallel bruises on the back, glutei and legs, Criss-cross contusions can be caused by sticks with a splayed end. These are accompanied with blunt trauma on the face and scalp causing swelling and racoon eyes. Fractures of the ulna, ribs and mandible and ecchymosis are often seen in such patients. Crush Syndrome and Sexual Assault can happen together.
These patients are brought to the Accident and Emergency Department by the police or by the community. They are all males and of the age group of 15 to 30 years. I haven’t seen any females with Sjambok injuries. They recover well after aggressive treatment in a multidisciplinary approach by Accident and Emergency Physicians, General Surgeons, Orthopaedic Surgeons, Radiologists and Pathologists take part. Unfortunately, there is no post trauma counselling. The article on Traumatic Rhabdomyolysis (Crush Syndrome) in the rural setting by Rosedale and Wood, published in the South African Medical Journal Vol 102, No 1 (2012), focuses on Sjambok Injuries and Crush Syndrome in patients seen in KwaZulu- Natal. [9]