Maksim Barsakov *Full member of the Society of Plastic, Reconstructive and Aesthetic Surgeons of Russia, Head of the Department of Plastic Surgery Pirogov Clinic, St. Petersburg, Bolshoy pr., Vasilievsky Island, Russia
* Correspondence: Barsakov Maksim, Department of Plastic Surgery, Pirogov Clinic, St. Petersburg, Bolshoy pr., Vasilievsky Island, Russia. Email: Barsakov@inbox.ru
Citation: Barsakov M, “Mastopexy with Dermal Fixation Personal Approach” J Aesthetic Surg Med 1 (2023): 104. DOI: 10.59462/JASM.1.1.104
Copyright: ©2025 Barsakov M. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribu- tion, and reproduction in any medium, provided the original author and source are credited.
A method for surgical treatment of mammary gland ptosis is described, which provides a filled upper pole of the mammary gland and a stable lower pole in the late postoperative period, which is optimal for the correction of severe ptosis with a vertical orientation of the nipple-areolar complex, which minimizes the need for extensive anchor sutures and preserves the possibility of lactation in the future. The technique is based on the method of forming an inferior or inferior-central dermo glandular pedicle, fixing the superior edge of the pedicle to the pectoral fascia or pectoralis major muscle with absorbable sutures using dermo muscular or dermo fascial attachment, and reducing the skin cover with a T-shaped or skin pattern with a J|L suture. The technical result is achieved by forming a lower or lower- central dermo glandular feeding pedicle, fixing the isolated axillary tail of the gland to the upper edge of the flap or resecting the axillary tail and, if necessary, part of the parenchyma of the upper part of the flap with further fixation of the dermal or dermo glandular upper edge of the feeding pedicle with three sutures to the pectoral fascia in the area of 10, 12 and 2 o’clock at the level of the planned position of the new upper slope of the mammary gland with preliminary detachment of the upper skin glandular flap in the superficial plane, subsequent dissection of the superficial fascia and the remainder of the gland of this flap with three radial incisions, cutting the skin and layer-by-layer suturing of the wound with the formation of an inverted T-shaped suture, J-suture or L-suture depending on the initial length of the lower slope of the gland and the direction of the nipple-areolar complex.
Testing of the technique in clinical conditions has shown the effectiveness of its use, ensuring the preservation of a more filled upper slope and stabilization of the lower slope of the mammary gland in the late postoperative period without significant complications after surgery in a large proportion of patients, as well as the absence of the need to use extensive anchor sutures even with severe ptosis of the mammary gland tissue.
Dermo glandular pedicle; Hypertrophic ptosis; Norm trophic ptosis; Inverted T-suture; Breast reconstruction; Mammoplasty; Mastopexy
The mammary gland maintains its normal position due to Cooper’s ligaments, which attach the glandular lobe to the superficial fascia of the skin and the pectoralis major fascia [1]. Ptosis of the mammary gland is directly related to the weakness of these ligaments and develops secondary to the pathogenic triad: progressive atony of the skin, downward displacement and stretching of the nipple-areolar
complex (NAC), and loss of fullness of the upper pole, which leads to a withering appearance of the mammary gland [2-4]. Ptosis can also be congenital or acquired-the former is caused by various genetic factors, while the latter is the result of pregnancy and lactation, or massive weight fluctuations. A high degree of ptosis can negatively affect a woman’s attractiveness and self-confidence [5-7].
Various mastopexy techniques are used in plastic surgery [8]. The degree of ptosis and the amount of tissue or volume of the breast are key factors that determine the surgical procedure, the choice of which is important and directly related to the outcome of the surgery. Mastopexy, commonly performed to correct breast ptosis, is the fifth most common procedure performed by plastic surgeons on women, with a significant increase of 31.4% in the frequency of this procedure worldwide from 2020 to 2021 [9].
Today, there are more than 600 methods for correcting ptotic breasts, but no more than 50 have become widespread [10-12]. The most frequently recorded complications are associated with either an increase in the number of scars or a loss of the final shape. While patients expect the best results with minimal scars and a short period of postoperative recovery [13-15]. In this regard, modern areas of mammoplasty are focused on the problem of reducing the number of skin scars and increasing the stability of the postoperative result. For this purpose, several different surgical strategies have been described, and almost all of them were based on the blood supply to the nipple and areola using a certain version of the upper pedicle [16-18]. But the problem of increasing the stability of filling the upper pole of the mammary gland and the stability of the shape of the lower pole in the late postoperative period remains unsolved [19] In this regard, the issue of developing the most optimal surgical strategy for the treatment of breast ptosis remains relevant.
Basics of mastopexy technique
The article describes a mastopexy technique patented in the Russian Federation (Patent for Invention No. 2808373 [20], which is aimed at solving the problem of the stability of the filling of the upper pole of the mammary gland and the stability of the shape of the lower slope in the late postoperative period. The technique was developed based on the SPAIR method proposed by Dennis Hammond [21], in which the lower dermo glandular pedicle is formed, fixed with absorbable sutures of the parenchyma to the pectoral fascia or pectoralis major muscle at the level of the 3rd rib and reduction of the skin cover by a circum-vertical cut with a J/L suture. But this method of reduction and lifting of mammary glands gives a poorly expressed fullness of the upper pole of mammary glands in the remote period due to the fact that the sutures fixing the gland tissue lose their strength and the cicatricial process in this case is unstable, the cut of the skin of the lower pole in the form of the letter J gives in the postoperative period more sagging compared to T-shaped and anchor cuts of the skin. Whereas it is necessary to preserve a more filled upper and stabilize the lower slope. It is precisely to eliminate these technical problems that the developed and tested technique of mastopexy is aimed.
Stages of the Mastopexy Technique
The purpose of the marking is to outline the zone of de-epidermisation of the dermo glandular pedicle and the future location of the NAC (Figure 1).
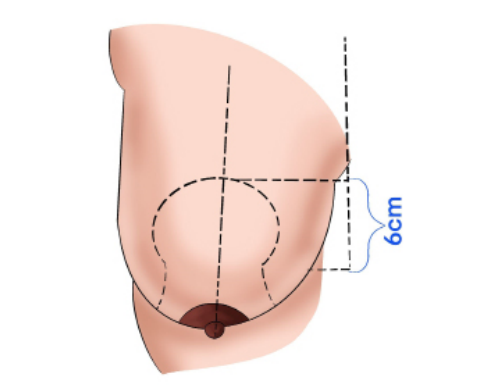
Figure 1. Marking the zone of de-epidermisation of the dermo
Skin marking is performed before the operation, when the patient is in a vertical position. The reference point for the upper edge of the marking is the projection of the level of the inframammary groove on the midline, and from this point we count upwards 5-6 cm (depending on the height and constitution of the patient). The patient is marked, as usual, for mastopexy using the vertical technique with the Lejour manoeuvre (Figure 1). Precise marking of all areas of skin excision is not required for this technique, since we mark the future excision zone only after we lift and fix the dermo glandular pedicle in a given position.
After de-epidermisation (Figure 2a), an incision in the dermis along the entire outer edge along the supraareolar zone of de-epidermisation is performed to form the inferior or inferior-central dermo glandular pedicle with preservation of the feeding vessels of the Würinger septum (Figure 2b).
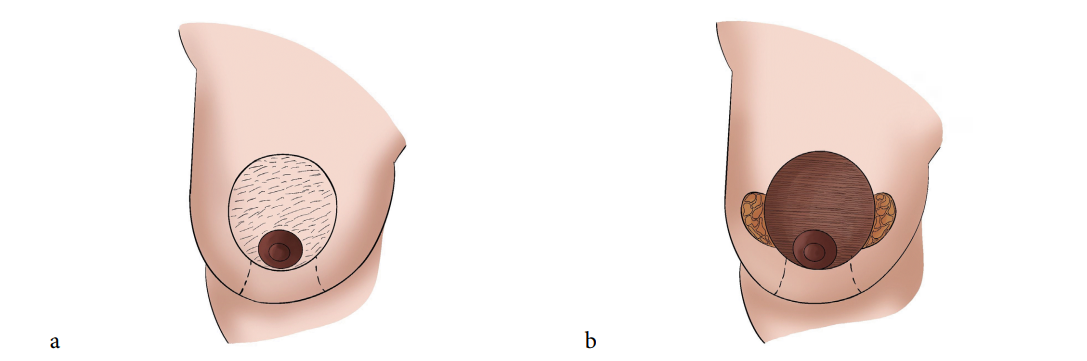
Figure 2 . Formation of the lower dermo glandular pedicle (a-de-epidermisation zone b- stage of formation of the lower dermo glandular pedicle
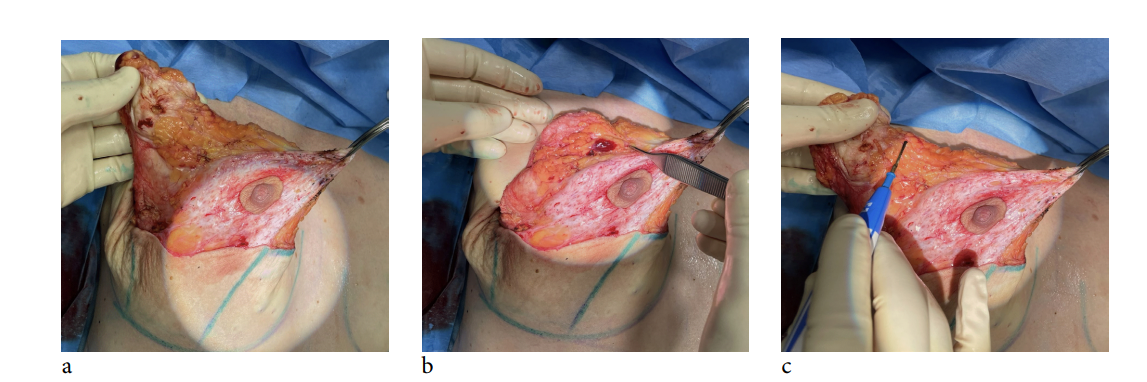
Figure 3a. The axillary tail of the mammary gland is isolated.
Figure 3b. Shows the mechanism of placing the tail on the upper edge of the dermo glandular pedicle with subsequent fixation (during mastopexy).
Figure 3c. Shows the stage of resection of the axillary tail (during reduction or correction of asymmetry).
Depending on the tasks set, either fixation of the isolated axillary tail to the upper edge of the dermoglandular pedicle (in mastopexy) or resection of the axillary tail in combination with resection of the tissue of the upper edge of the pedicle (in reduction or correction of asymmetry) is performed. Removal of the axillary tail of the gland in combination with resection of the lateral edge of the isolated dermoglandular pedicle ensures a reduction in the width of the mammary gland, which is beneficial in the case of its reduction (Figures 3a-3c).
Next, the dermal or dermoglandular flap of the upper free edge of the pedicle is fixed with three sutures of absorbable suture material to the pectoral fascia in the area of 10, 12 and 2 o’clock at the level of the planned position of the new upper pole of the mammary gland with preliminary detachment of the upper skin glandular flap in the suprafascial plane (Figures 4a and 4b).
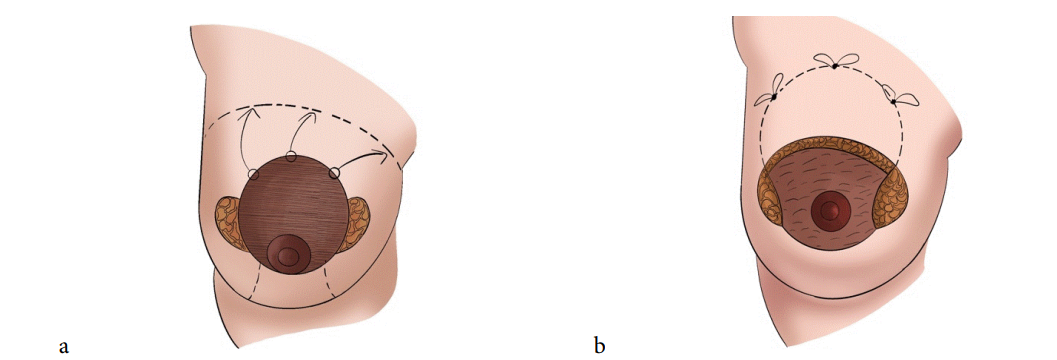
Figure 4. Fixation of the dermal or dermoglandular flap of the free upper edge of the pedicle
The fixation of the dermoglandular flap to the pectoral fascia occurs due to the dermal component (the strength of the cicatricial dermofascial junction is higher than the glandular-fascial junction) (Figure 5). A drainage system is installed if necessary (in case of severe tissue bleeding or in case of massive reduction) under the flap and subsequent temporary sutures are applied with non-absorbable suture material or a stapler on the vertical and horizontal components to obtain the shape and determine the zone of future de-epidermization in the area of the lower pole of the breast.
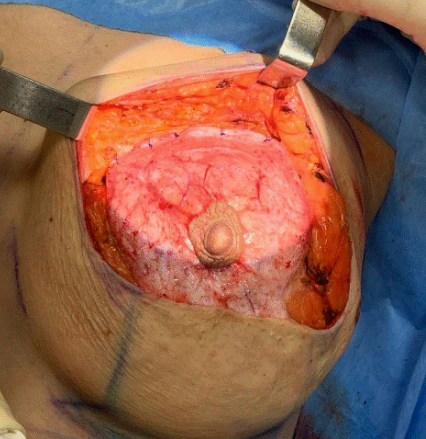
Figure 5. Fixation of the upper edge of the dermoglandular pedicle to the pectoral muscle
Drawing the lines of the future de-epidermization zone is carried out before removing the temporary sutures. Then de-epidermization is carried out according to the markings in the area of the lower slope and subsequent dissection of the dermis along the entire perimeter of de-epidermization. (Figure 6). Layer-by-layer suturing of the wound is carried out with the formation of an inverted T-shaped suture or J/L-suture. The choice of the type of skin cut depends on the initial length of the lower slope of the gland and the direction of the NAC.
Stabilization of the lower pole is achieved by a T-shaped skin pattern, which allows for a reduction in the length of the formed lower pole of the mammary gland (Figure 7).
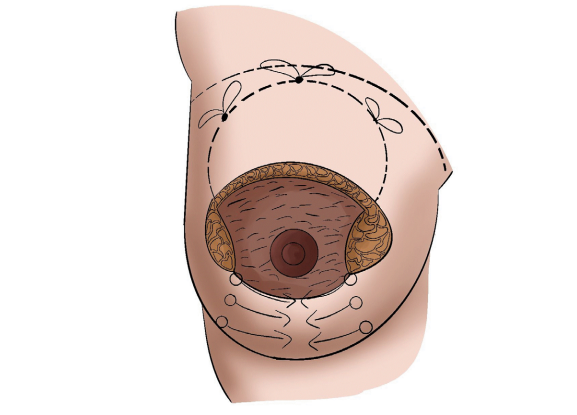
Figure 6. Application of temporary sutures to the skin of the lower pole to determine the zone of de-epidermization
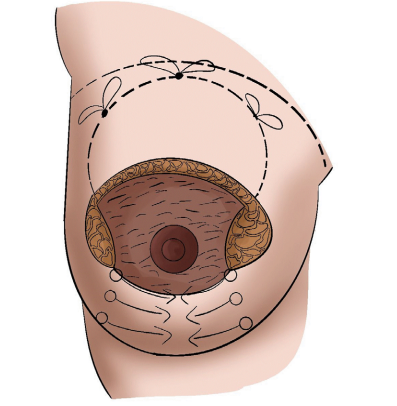
Figure 7. Suturing the skin in the area of the lower pole after de-epidermization
Next, layer-by-layer suturing of the periareolar region is performed with the application of a round blocking suture (non-absorbable monofilament thread 3.0) (Figures 8a-8c)
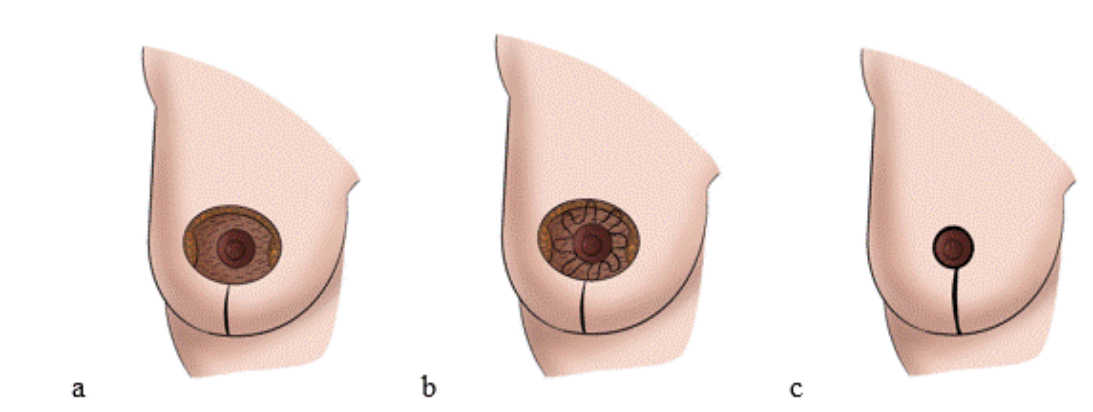
Figure 8(a-b-c). Stages of suturing the periareolar region with the application of a round blocking suture.
Pirogov Clinic from January 2016 to June 2022.
Using the developed surgical technique, 152 patients with breast tissue ptosis aged 23 to 51 years were operated on at the Department of plastic surgery of (Figures 9a-9c) shows the results of surgical correction of mammary gland ptosis using the stated method.
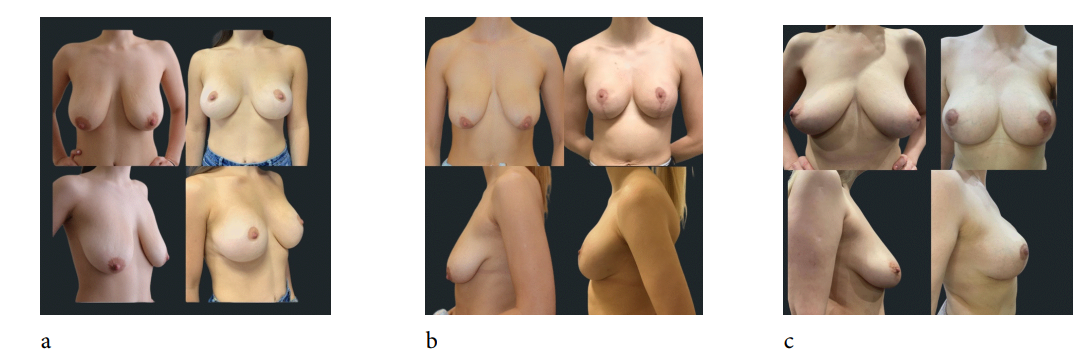
Figure 9. Results of using the described surgical technique for correcting ptosis of the mammary glands.
a - Patient I., 29 y.o., complained of breast ptosis after childbirth. A mastopexy was performed with a T-shaped skin pattern. Result after 1 year.
b - Patient H., 24 y.o., complained of breast ptosis after childbirth and massive weight loss.
Mastopexy was performed using the specified technique with J/L-shaped skin pattern. Result after 6 months
c- Patient E., 36 y.o., complained of aesthetic dissatisfaction with the shape of her breasts, ptosis.
Pregnancy-1. Childbirth-1. No weight fluctuations. Mastopexy was performed using the specified technique with a T-shaped skin cut. Result after 6 months
(Figures 10a,10b) shows the results of surgical correction of ptosis with elements of reduction of the volume of breast tissue using the stated method.
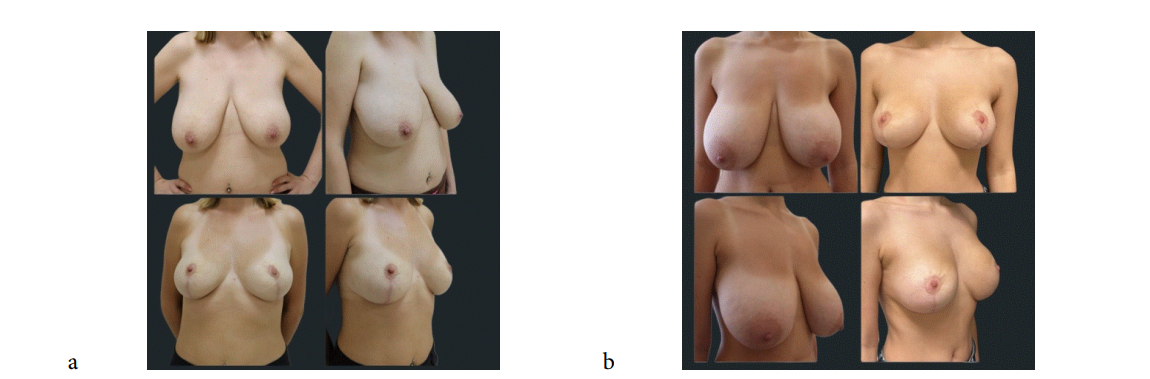
Figure 10. Results of using the described technique for surgical correction of ptosis with elements of reduction.
A-Patient M, 49, complained of ptosis and large breast size. She had two births in her anamnesis. A mastopexy was performed with a reduction of 300 grams of glandular tissue on each side using the specified technique with a T-shaped skin cut. The result after 6 months
B-Patient A., 29, complained of ptosis and large breast size. She had one birth in her anamnesis. Mastopexy was performed with reduction of 600 g of glandular tissue on each side using the specified technique with a T-shaped skin pattern. Result after 4 months.
In total, during the entire observation period, postoperative complications occurred in the amount shown in absolute and percentage terms in Table 1. The quantitative distribution of complications identified during observation of patients after mastopexy is presented in (Table 1).
| Complication | Abs. qty. | Fractional qty |
|---|---|---|
| Deterioration of healing of the junction of vertical and horizontal sutures | 18 | 10.23 |
| Permanent loss of sensitivity of the NAC | 2 | 1.14 |
| Deterioration of vertical suture healing | 7 | 3.98 |
| Instability of the shape of the mammary gland | 7 | 3.98 |
| Ischemia, necrosis of the NAC | 0 | 0 |
Table 1. Complications identified during observation of patients after correction of mammary gland ptosis using the described technique
Thus, deterioration of healing of the junction of the vertical and horizontal sutures within 1-1.5 months after surgery was recorded in 10.2% of patients. It should be noted that with ointment therapy, healing in the majority of patients was observed within 7-20 days. Permanent loss of sensitivity of the NAC was recorded in 2 cases (1.13%) (on the right). In 3.9% of cases, deterioration of healing of the vertical suture was detected, but conservative treatment ensured healing with minimal aesthetic defects. Instability of the shape of the mammary gland in the postoperative period (with observation for 6-12 months) was detected in 3.9% of cases. This complication was probably associated with the fatty type of structure of the mammary glands. Vascular disorders in the NAC area or areola necrosis were not recorded throughout the observation period. In the late postoperative period, 5 (2.8%) patients became pregnant. After the birth of the child, no problems arose among the patients during lactation.
A retrospective-prospective analysis was conducted by means of a questionnaire survey of 150 women aged 23-50 years after they had undergone reduction mastopexy using the described technique in periods from 3 months to 1 year. The questionnaire survey was anonymous and voluntary, and was conducted free of charge. The analysis allowed us to identify the degree of patient satisfaction with the form and stability of the result obtained.
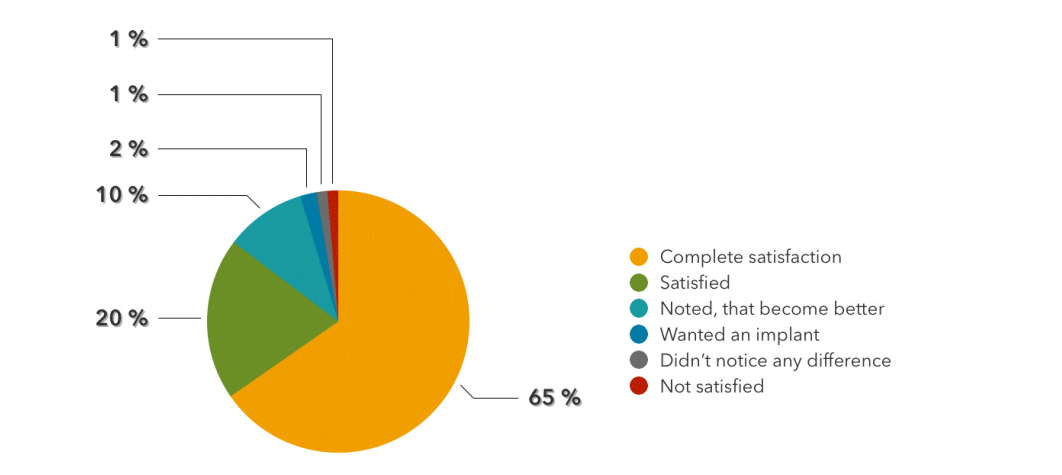
Figure 11. Patient satisfaction level with the resulting breast shape after surgery using the described technique.
Of the 150 respondents, 98 (65%) women reported complete satisfaction with the resulting shape and stability of their breasts, which exceeded their expectations; 30 (20%) were satisfied with the new shape and position of their breasts; 15 (10%) noted that their breasts had become better in shape, but not as they had imagined; 3 (2%) wanted to install a silicone implant without achieving the desired
stability; 2 (1.3%) did not notice any difference from the original shape and position of their breasts; 2 (1.3%) were not satisfied with the new shape of their breasts (Figure 11).
Analysing the results of using this technique, the author concluded that this technique is well suited for correcting grade 3 ptosis (according to Renault), when the position of the NAC is directed as downwards as possible (Figure 12a), explaining that the movement of the entire gland-NAC complex looks more logical than the formation of an upper or upper-medial feeding pedicle of the NAC with a long distance (Figure 12b). This technique is quite simple to perform, allows for controlled lifting of the gland flap to the desired position, giving the upper pole a more filled appearance. Fixation of the dermoglandular pedicle occurs by dermo-muscular-fascial sutures, which is a more durable method compared to fixation of only glandular tissue (in the SPAIR technique, fixation of the pedicle occurs by muscular-glandular sutures, which is a less durable method) [21]. Detachment and movement of the gland flap also ensures narrowing of the base of the breast, which has a beneficial effect on the aesthetic perception of the shape. By preserving the gland mass and its connection with the NAC, we minimize the risks of ischemic complications and ensure the potential possibility of lactation in the future. In addition, this technique allows us to avoid community anchor scars even with pronounced ptosis.
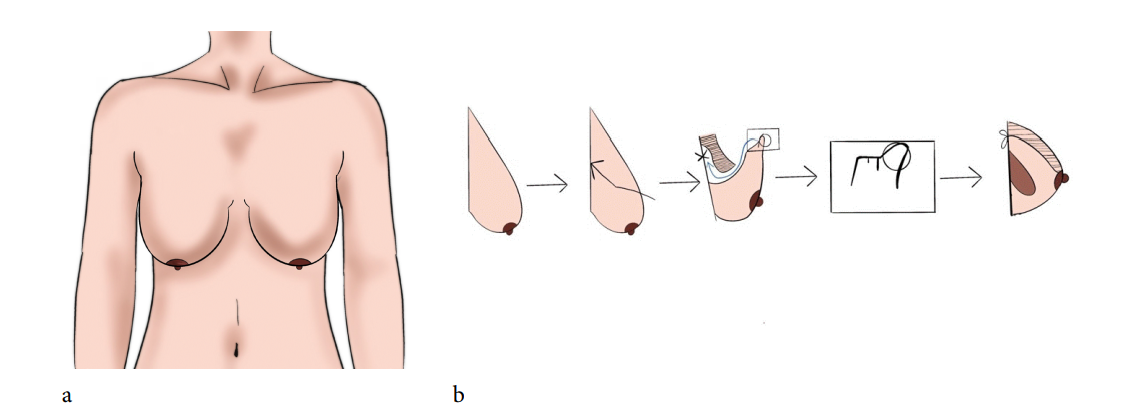
Figure 12. Schematic representation of the ptosis of the mammary gland, optimally suitable for the application of the described surgical technique (in the author’s opinion). a-photo from the front. b-photo from the side. Schematic representation of the lifting and movement of the gland flap during the described technique.
Thus, the advantages provided by the described technique of surgical treatment of ptosis of the mammary glands include the formation of a more filled upper pole and a stable lower pole in the late postoperative period, which is manifested in the satisfaction of patients with the new shape of the resulting breast. In the author’s opinion, the technique is recommended for the correction of grade 3 ptosis (according to Renault) with the position of the NAC maximally seasoned downwards.
All procedures performed in studies involving human participants were in accordance with the Declaration of Helsinki (revised 2013). Informed consent was obtained from patients for publication of this manuscript and any accompanying images.
[1] Martinez, Amaury A., and Susan Chung. “Breast ptosis.” (2021)
[2] See, Mee-Hoong, Kah-Chun Yip, Mei-Sze The and Lee-Lee et al. “Classification and assessment techniques of breast ptosis: A systematic review.” Plast Reconstr Aesthet Surg (2023): 380-395
[3] Alcocer, Giovanni, Priscilla Alcocer, and Carlos Marquez. “Effect of the Gravity on the Sagging Breasts of Women.” Asian Journal of Applied Science and Technology 3 (2020): 167-182
[4] Wong, Corrine, Megan Vucovich, and Rod Rohrich. “Mastopexy and reduction mammoplasty pedicles and skin resection patterns.” Plastic and Reconstructive Surgery– Global Open 8 (2014): 202
[5] Caliri, Andrew W., Stella Tommasi, and Ahmad Besaratinia. “Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer.” Mutation Research/Reviews in Mutation Research 787 (2021): 108365
[6] 6. Alessandri Bonetti, Mario, Riccardo Carbonaro, Francesco Borelli, and Francesco Amendola et al. “Outcomes in hybrid breast reconstruction: a systematic review.” Medicina 9 (2022) 1232.
[7] 7. Uribe, Laura C. Cala, Mauricio Perez Pachon, Andres Villate Hernandez, and Andreina Zannin Ferrero. “Kite Mastopexy: Small Scar and Tissue-conserving Technique.” Plastic and Reconstructive SurgeryGlobal Open 9 (2023): e5265
[8] Wagner, Ryan D., Jeffrey L. Lisiecki, Michael V. Chiodo, and Rod J. Rohrich. “Longevity of ptosis correction in mastopexy and reduction mammaplasty: a systematic review of techniques.” JPRAS open 34 (2022): 1-9
[9] Serson, David. “International society of aesthetic plastic surgery.” (1970): 528
[10] . Spear, Scott L, and Michael A. Howard. “Evolution of the vertical reduction mammaplasty.” Plastic and reconstructive surgery 3 (2003): 855-869
[11] Hall-Findlay, Elizabeth J. “Pedicles in vertical breast reduction and mastopexy.” Clinics in plastic surgery. 3 (2002): 379-391.
[12] Rohrich, Rod J., Amanda A. Gosman, Spencer A. Brown and Prasanthi Tonadapu et al. “Current preferences for breast reduction techniques: a survey of board-certified plastic surgeons 2002.” Plastic and reconstructive surgery. 7 (2004): 1724-1733
[13] Wagner, Ryan D., Jeffrey L. Lisiecki, Michael V. Chiodo, and Rod J. Rohrich. “Longevity of ptosis correction in mastopexy and reduction mammaplasty: a systematic review of techniques.” JPRAS open. 34 (2022): 1-9
[14]Panayi, Adriana C., Riaz A. Agha, Brady A. Sieber, and Dennis P. Orgill. “Impact of obesity on outcomes in breast reconstruction: a systematic review and meta-analysis.” Journal of reconstructive microsurgery. 5 (2018): 363-375
[15] Li, Shangshan, Dali Mu, Chunjun Liu, Minqiang Xin and Su Fu, Boyang et al. “Complications following subpectoral versus prepectoral breast augmentation: a meta-analysis.” Aesthetic Plastic Surgery. 43 (2019): 890-898
[16] Zucal, Isabel, Mathias Tremp, Dominik Duscher and Raphael Wenny et al. “Augmentation-mastopexy: analysis of 95 consecutive patients and critical appraisal of the procedure.” Journal of Clinical Medicine. 9 (2023): 3213.
[17] Wall, Holly C., Sameer H. Halani, Chizoba Mosieri and Charles et al. “Tension reduction with Force modulating tissue bridges reduces wounds in breast surgery.” Aesthetic Surgery Journal. 12 (2023): 1471-1480.
[18] Kim, Dylan K., Grant B. Feuer, Paige E. Warner, and Jeffrey A. Ascherman. “Predictors of extended length of stay following outpatient reduction mammaplasty.” Journal of Plastic, Reconstructive & Aesthetic Surgery. 94 (2024): 141- 149
[19] di Summa, Pietro G., Carlo M. Oranges, William Watfa and Gianluca Sapino et al. “Systematic review of outcomes and complications in nonimplant-based mastopexy surgery.” Journal of Plastic Reconstructive and Aesthetic Surgery. 6 (2019): 1049-1049
[20] . Method of surgical treatment of normotrophic and hypertrophic ptosis of the mammary glands of 2 or 3 degree
[21] Hammond, Dennis C. “The short scar periareolar inferior pedicle reduction (SPAIR) mammaplasty.” In Seminars in plastic surgery, vol. 18, no. 03, pp. 231-243. Copyright© 2004 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001 USA., 2004.