Fabrizio Chirico 1 *, Gianpaolo Tartaro 1 , Luigi Rugge 2 , Ciro Emiliano Boschetti 1 , Salvatore D’Amato 1 , Ivo Ferrieri 1 , Mario Santagata 1
1Maxillofacial Surgery Unit, Multidisciplinary Department of Medical-Surgical and Dental Specialities, University of Campania “Luigi Vanvitelli”, 80138 Naples, Italy.
2 Private Practice, 80136 Naples, Italy
* Correspondence: Fabrizio Chirico, Maxillofacial Surgery Unit, Multidisciplinary Department of Medical-Surgical and Dental Specialities, University of Campania “Luigi Vanvitelli”, 80138 Naples, Italy; E-mail: fabriziochirico@hotmail.com
Citation: Chirico Fabrizio, Tartaro Gianpaolo, Rugge Luigi, and Boschetti Ciro Emiliano, et al. “Minimally Invasive Approach for Buccal Fat Pad Transposition in Orthofacial Surgery.” J Aesthetic Surg Med (2023): 102. DOI: 10.59462/JASM.1.1.102
Copyright: © 2023 Chirico F, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Modern approach in orthofacial surgery focus on enhancing not only dentoskeletal discrepancies but contextually facial aesthetic refinement [1-6]. In case of skeletal disharmony and concave profile, Le Fort I osteotomy for maxillary advancement could result in dissatisfaction for midface contour flattening that could become more evident postoperatively. Thus, midface irregularities in orthofacial surgery are absolutely a paramount topic for the maxillo-facial surgeon that should refer to the most suitable approach to enhance outcomes and satisfaction rates, as patient specific implants (PSI), osteotomy lines modification and facial soft tissue contouring as Bichat paddle or buccal fat pad (BFP) grafting. Thus we describe our experience to succeed midface aesthetic improvement in orthofacial surgery by a novel approach in BFP transposition.
From December 2020 to December 2022, 18 consecutive nonsyndromic patients underwent BFP transposition as a procedure in combination with bimaxillary surgery and genioplasty at the author’s center [7]. A modified BFP transposition protocol was followed. Guidelines from the Declaration of Helsinki were followed at all treatment phases. After the 6 months period, a retrospective evaluation of patients who underwent this surgical protocol was performed. The studied sample consisted of 10 women and 8 men. Average age 30.6 years.
Subjective evaluation was performed by the assessment of patients and surgeon postoperative satisfaction with the resulting volumetric outcome regarding depression filling, facial symmetry and the overall aesthetic improvements 6 months postoperatively. A visual analogue scale (VAS) was rendered ranging from 0 to 10 was used in case of satisfaction, 0 meant complete dissatisfaction and 10 meant maximum satisfaction.
A modified BFP transposition protocol was followed. The mean surgical time of the surgical procedure was 15 minutes (range, 10–25 minutes) and all 18 patients were operated under general anaesthesia by the same surgeon (M.S.).
Through the minimally invasive approach (from region 1.3 to region 2.3) for Le Fort I osteotomy (Figure 1), a subperiosteal flap was raised over the malar antero-lateral side. Thus, careful dissection of the buccal fat pad was performed with facial nerve branches preservation (Figure 2).
An 18-gauge needle was inserted through the skin-point M (point of maximum malar projection) and exited through the fibroareolar tissue. A 4/0 absorbable suture without a needle was inserted through this needle from the oral cavity to the outside. The needle was retracted through
the BFP transposition and enhance a smooth transition of the naso-malar groove. The same procedure was done through point S in the contralateral side to achieve symmetry for a surgical intraoperative mirroring in malar augmentation.
No post-operative local and general complications are reported. No surgical complications infection and need for revision occurred. Facial appearance scores after procedure were subjectively better than scores before surgery at VAS evaluation also in cases of large maxillary advancement (Figure 4-5-6). During the 6 months follow-up period, no graft resorption occurred thus were considered to be unnecessary any overcorrection with the resulting facial symmetry and volume enhancement.
point M without leaving the skin entry point, then returned to the oral cavity in a more medial position through the same entry point. Finally, the needle was retracted from point M leaving the suture through the soft tissues to the oral cavity without any cutaneous hollowing. The fixed malar point was the vehicle to the exact transposition of the BFP in malar augmentation. This suture was the key point to led through the same entry port toward the malar pocket and to achieve the engagement of the buccal fat pad subperiosteally. The progression of the suture allowed for displacement of the buccal fat pad toward the uppermost and lateral areas of the pocket. A notch was made in the fibrous component of Bichat paddle and raised in the desired position. Finally, a double knot secured the flap into the appropriate position: stabilization suture in 4/0 absorbable suture was made in proximity of the maxillary titanium medial and lateral plate (Figure 3) to uniformize
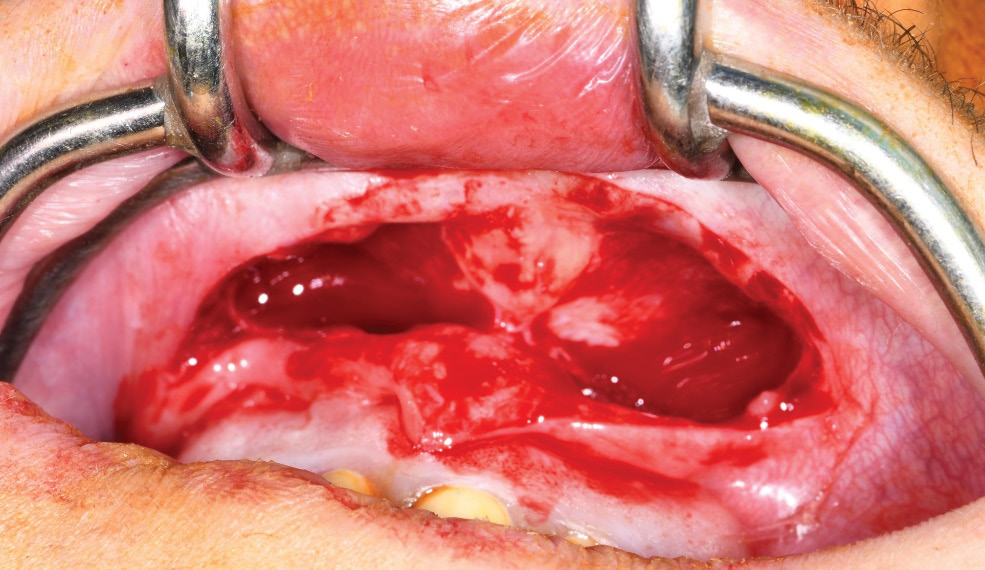
Figure 1. Minimally invasive approach for Le Fort I osteotomy.
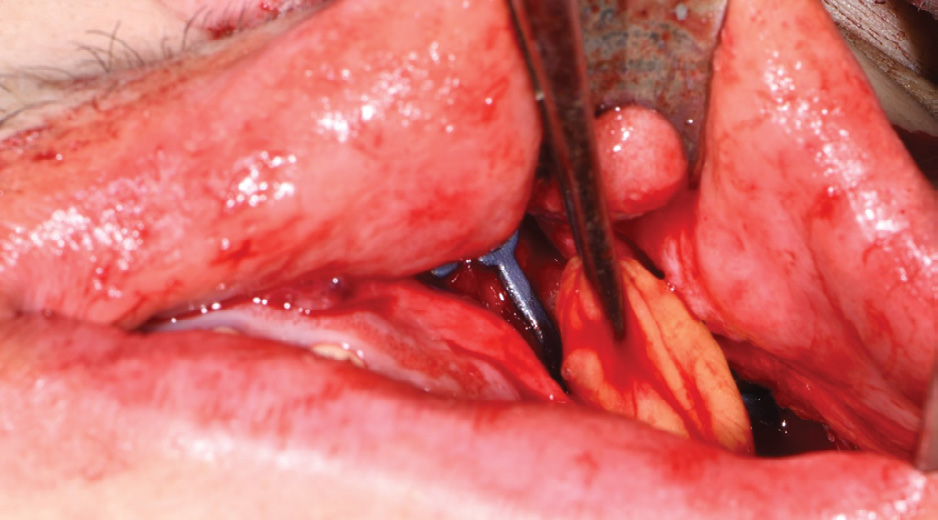
Figure 2.Buccal fat pad dissection and transposition
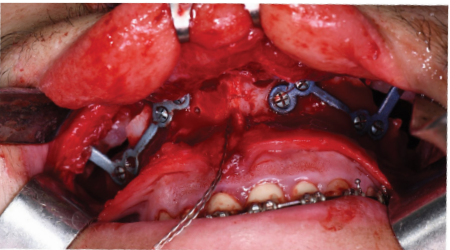
Figure 3.Custom made plates for rigid fixation after maxillary advancement.
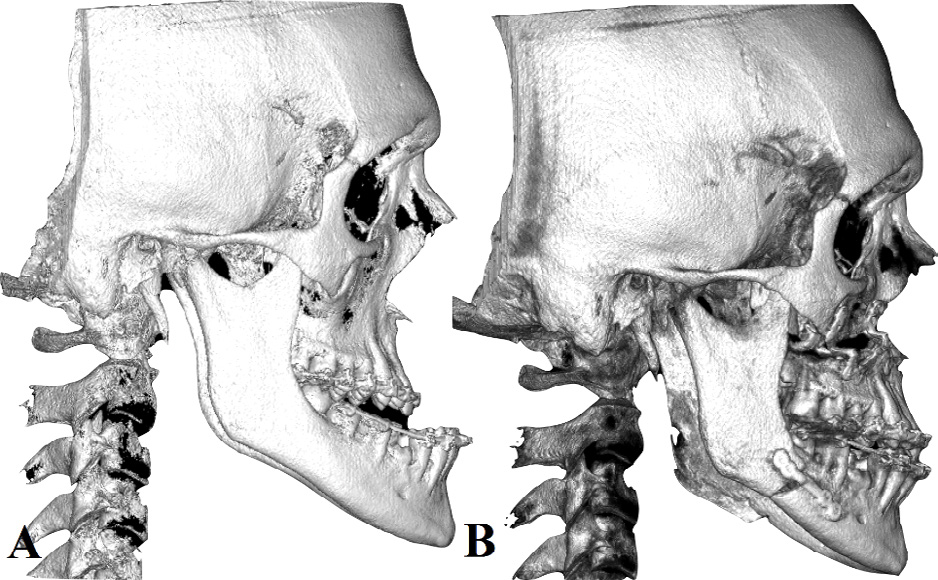
Figure 4.A – B. Pre and post-operative imaging of double jaw orthofacial surgery

Figure 5.A – B. Pre and post-operative frontal view of patient who underwent BFP transposition contextually to orthognatic surgery. The increasing of midface volume and the smoothened transition of malar-midface regions is emphasized.
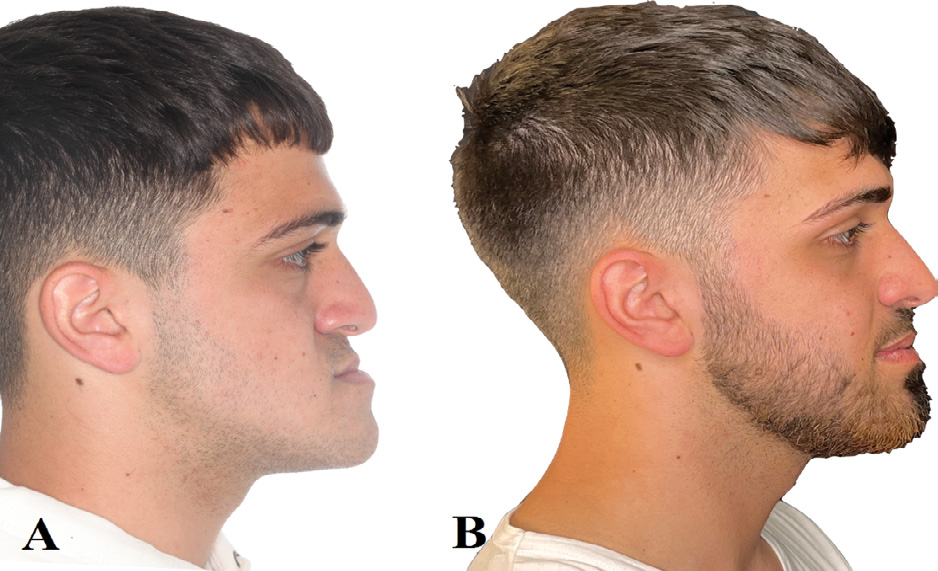
Figure 6.A – B. Pre and post-operative lateral view of patient who underwent BFP transposition. The volumetric increasing of midface and the smoothened transition of nasal-midface regions is highlighted.
Current aspects of orthofacial surgery focus on aesthetic enhancement as one of the core topic to determine the success in modern orthognatic surgical procedure [8-10]. Moreover, our technique underlines as the cheek region is an important element to be considered in surgical planning. In this regard, our approach has beneficial effect both on facial appearance-related perception and volumetric improvement of the malar area. For this, preoperative diagnosis and surgical planning should be delineated by analysing facial aesthetic as contours proportions and symmetry of facial units, in addition to the occlusion reassessment that is typically the main target of traditional orthognatic surgery.
The characteristics of buccal fat pad as complete biocompatibility, versatility, availability and improvement of tissue quality in addition to the minimal invasivity of our approach and the stability of the results allow that this synchronous procedure not only increases midface volume but also produces a smoothened transition of the nasal-midface and malar-midface regions.
The buccal fat pad contains a rich bloody supply and high mesenchymal cells concentration and has the main advantage to avoid external incisions and proximity to the augmented site thus a low harvesting donor-site morbidity. However, the surgeon should have experience with buccal fat pad flaps according to the detailed anatomy of facial nerve buccal branches and vessels.
Our modified and minimally invasive BFP transposition is a simple and fast recovery procedure, with the possibility of discharge on the first postoperative day, besides presenting a low cost. Moreover, this surgical technique is safe, tailored to the size of the planned volumetric augmentation and it is associated with minimal postoperative complication and minimal donor site morbidity.
According to our experience, the aim of our modified approach in pedicled buccal fat pad transposition is to perform surgical reshaping in midface area avoiding the disadvantages of the conventional techniques. Moreover, our modified technique allows the avoiding of skin hollowing in the needle entry point as described in other approaches described in literature.
We prefer to achieve the buccal fat pad mobilization contextually to orthofacial surgery in selected cases as concave or flat profile because our approach results in cheek hollowing thus an aesthetic emphasization of the malar projection.
Our modified technique represents an excellent tool for malar augmentation in patients in whom an orthofacial surgery is planned. In fact, Le Fort I approach allows for easy dissection and buccal fat pad upper repositioning. The technique is safe and fast, with the advantage of a minimally invasive approach that could be performed contextually to orthofacial surgery and is associated with minimal morbidity and high patient satisfaction.
[1] Hernández-Alfaro, Federico, and Adaia Valls- Ontañón. “Aesthetic Considerations in Orthofacial Surgery.” Oral Maxillofac Surg Clin 35 (1) (2023): 1-10.
[2] Jansma, Johan, and Rutger H. Schepers. “Adjunctive Aesthetic Procedures in Orthognathic Surgery.” Oral Maxillofac Surg Clin 35 (1) (2023): 139-152.
[3] Wu, Robin T., Alexander T. Wilson, Cyril S. Gary, and Derek M. Steinbacher. “Complete reoperation in orthognathic surgery.” Plast Reconstr Surg 143 (5) (2019): 1053e-1059e.
[4] Li, Dion Tik Shun, and Yiu Yan Leung. “Patient- Specific Implants in Orthognathic Surgery.” Oral Maxillofac Surg Clin 35 (1) (2023): 61-69.
[5] Mohamed, Waheed V., and Jon D. Perenack. “Aesthetic adjuncts with orthognathic surgery.” Oral Maxillofac Surg Clin 26 (4) (2014): 573-585.
[6] Raffaini, M., and C. Pisani. “Orthognathic surgery with or without autologous fat micrograft injection: Preliminary report on aesthetic outcomes and patient satisfaction.” Int J Oral Maxillofac Surg 44 (3) (2015): 362-370.
[7] Santagata, Mario, Salvatore D’Amato, Ivo Ferrieri, Annalisa Pollice, Pasquale Verolino, Ciro Emiliano Boschetti, and Gianpaolo Tartaro. “A Modified of Bilateral Sagittal Split Osteotomy: Technical Note and Proposal of a Nomenclature on the Osteotomy Lines.” Arch Craniofac Surg 34 (3) (2023): e306-e308.
[8] Posnick, Jeffrey C., Mihai Radulescu, and Brian E. Kinard. “Redo orthognathic surgery: A report of 10 cases.” Oral Surg Oral Med Oral Pathol Oral Radiol Endod 127 (6) (2019): 477-489.
[9] Tozzi, U., M. Santagata, A. Sellitto, and G. P. Tartaro. “Influence of kinesiologic tape on post-operative swelling after orthognathic surgery.” J Oral Maxillofac Surg 15 (1) (2016): 52-58.
[10] Santagata, Mario, Nicola Sgaramella, Fabrizio Chirico, Salvatore D’Amato, Ivo Ferrieri, Giovanni Corvo, Camilla Corvo, and Gianpaolo Tartaro. “W-Shaped Osteotomy to Avoid Paranasal Deformity After Standard Le Fort I in Orthognathic Surgery.” Plast Reconstr Surg 30 (1) (2022): 45-48.