Michelle Christina 1 *, Riya Lal 2 , G. Mrudul Manoj 3 and Rajiv Choudhrie 4
1,2,3,4 Department of Surgery, Padhar Hospital, Betul, Madhya Pradesh, India
* Correspondence: Michelle Christina, Department of Surgery, Padhar Hospital, Betul, Madhya Pradesh, India, LCCU, Padhar hospital, Padhar, Betul district, Madhya Pradesh, India- 460001, Email: mich7george@ gmail.com
Received: 10 November 2023; Accepted: 24 November 2023; Published: 04 December 2023
Citation: Christina Michelle, Lal Riya, Manoj Mrudul and Choudhrie Rajiv. “Surgical Approach to a Case of Recurrent Oral Submucosal Fibrosis in a Rural Area of Central India.” J Aesthetic Surg Med (2023): 101. DOI: 10.59462/JASM.1.1.101
Copyright: © 2023 Christina M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Oral Submucosal Fibrosis (OSMF) is a premalignant condition that is a chronic, insidious, and incapacitating disease of the oral mucosa and oropharynx, occasionally occurring in the larynx. We bring to you a case of recurrent oral submucosal fibrosis in a 37-year-old male who presented with a gradual decrease in the extent of mouth opening. On local examination his interincisal distance was nil and there was extensive posterior buccal mucosa fibrosis bilaterally. Even after 2 previous interventions, the recurrence of his disease was high, also there is a high chance of malignant transformation thus a surgical approach was decided for him. When such a case presents to the hospital which has multiple failures of previous interventions it needs to be approached with caution and the management needs to be decided based on the benefit and the patients’ financial background and the prognosis of the intervention.
Oral Submucosal Fibrosis (OSMF) is a premalignant condition of the oral mucosa and oropharynx, occasionally occurring in the larynx [1]. It was first reported in 1952, by Schwartz in five Indian women from East Africa, while in 1953 a report by Joshi described the term “submucous fibrosis” of the palate and pillars [2]. We bring to you a case of recurrent oral submucosal fibrosis and the management used in a rural area of India.
Mr. X an average-built gentleman, presented with gradual decrease in the extent of mouth opening. The patient was a known tobacco chewer for the past 25 years and was diagnosed with OSMF stage 4 at another surgical center for which he underwent release of fibrous bands and
reconstruction of defects with palatal flaps, however, had a recurrence and presented to our hospital. On examination his interincisal distance was nil and there was extensive posterior buccal mucosa fibrosis bilaterally, the contour of the lips was normal and no changes in the angle of the mouth were noted. CT findings were suggestive of asymmetrical mucosal thickening of the bilateral buccal mucosa. The X-ray revealed a bilateral coronoidectomy defect. A thorough investigation and pre-anesthetic workup was done.
Tracheostomy was performed under LA and the patient was induced. A 2-team approach was planned. Fibrous bands were released trans-orally from the left to the right commissure of the lip and across the soft palate as well. Inter-incisional distance of 45mm was achieved using a heister mouth gag. Wiring of Tooth numbers 41, 42, 43 and 44 was done. A radial artery forearm free flap was placed on the left and right buccal mucosa extending
Following discharge, on his weekly visits his mouth opening exercises were done. On his 4 th month review visit his mouth opening was measured as 35 mm.
OSMF is characterized by juxta-epithelial inflammation followed by a chronic change in the fibro elasticity of lamina propria and epithelial atrophy. This results in a burning sensation, blanching, and stiffening of oral mucosa and oropharynx leading to restricted mouth opening [2]. The aetiological factors are chewing areca-nut [3], others include capsaicin in chilies, iron, zinc, and essential vitamin deficiencies [2].
The staging of OSMF can be done by the following criteria given first by More et al.
Clinical staging:
Stage 1– Stomatitis and/or blanching of the oral mucosa.
Stage 2 – Presence of palpable fibrous bands in buccal mucosa and/or oropharynx, with/without stomatitis
Stage 3 – Presence of palpable fibrous bands in buccal mucosa and/or oropharynx, and any other parts of the oral cavity, with/without stomatitis.
Stage 4 A. Any one of the above stages along with other potentially malignant disorders e.g., oral leucoplakia, oral erythroplakia, etc. B. Any one of the above stages along with oral carcinoma [2].
Functional staging: Inter-incisal mouth opening
M1: >35 mm.
M2: 25 mm and 35 mm.
M3: 15 mm and 25 mm.
M4: <15mm. 2
across the palate, donor site needed an STSG. The radial artery was anastomosed with the left facial artery to sustain the arterial supply and the cephalic vein to the left facial vein. Postoperatively the patient was kept in HDU and hourly monitoring of the flap was done. He was found to have transient left facial nerve palsy on post-op day 1 and was started on nerve stimulation therapy, however, the flap perfusion appeared satisfactory. Tracheostomy was decannulated on post-op day 10. The patient was monitored in the ward and was stable thus his sutures were removed and was discharged .
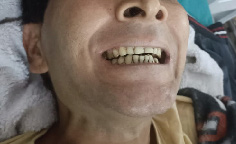
Figure 1. Pre-operative picture

Figure 2. Intra-operative picture
Management of the cases depends on the stage and extent of the disease. In our case, taking into consideration the extent of his mouth opening and the structures involved he was diagnosed with stage 4 OSMF. Due to Multiple recurrences and a high chance of malignant transformation surgical approach was decided for him. The advantage of this procedure is an increase in vascularity, reduced risk of contracture, faster healing, and low donor site comorbidities while the disadvantage is that the flap is bulky thus the patient is not able to clench his teeth and a secondary debulking procedure might be needed.
When such a case presents to the hospital which has multiple failures of previous interventions the management needs to be decided based on the patient’s financial background and the prognosis of the intervention. Delayed presentations and recurrent disease need a radical release of fibrous tissue and resurfacing with vascular flaps also aggressive post-op physiotherapy are mandatory.
[1] 1. Pindborg, Jens J., and Satyavati M. Sirsat. “Oral submucous fibrosis.” Oral Surg 22 (6) (1966): 764-779.
[2] 2. More, Chandramani B., Sunanda Das, Hetul Patel, Chhaya Adalja, Vaishnavee Kamatchi, and Rashmi Venkatesh. “Proposed clinical classification for oral submucous fibrosis.” Oral Oncol 48 (3) (2012): 200-202.
[3] 3. Sinor, P. N., P. C. Gupta, P. R. Murti, R. B. Bhonsle, D. K. Daftary, F. S. Mehta, and J. J. Pindborg. “A case-control study of oral submucous fibrosis with special reference to the etiologic role of areca nut.” J Oral Pathol Med 19 (2) (1990): 94-98.