Ravi Kumar Chittoria1*,Kanav Gupta22,Nagarjun S Ghatti3
1Senior Professor and Associate Dean (Academic), Head of IT Wing and Telemedicine Department of Plastic Surgery and Telemedicine JIPMER, Puducherry, India
2Senior Resident Department of Plastic Surgery JIPMER Puducherry,India
3Observer, Department of Plastic Surgery JIPMER Puducherry, India
Received: 18 Nov 2025;Accepted:04 Dec 2025; Published:12 Dec 2025;
Citation:Ravi Kumar Chittoria, Kanav Gupta, Nagarjun S Ghatti.“Colorado Needle Assisted Full Thickness Skin Graft Harvest.” J Aesthetic Surg Med (2025): 109. DOI: 10.59462/3068-5311.2.1.109
Copyright: © 2025 Ravi Kumar Chittoria..This is an open-access arti cle distributed under the terms of the Creative Com mons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Electric burn injuries most commonly occur in household or workplace settings and frequently involve the hand, as it is usually the point of contact with the electrical source. Management requires a staged approach including resuscitation, monitoring, serial debridement, and definitive reconstruction based on defect characteristics. Coverage options include local flaps, distant flaps, biological substitutes, and free flaps for complex defects. Skin grafts serve either as intermediate coverage prior to flap reconstruction or as definitive cover in selected cases. The Colorado microdissection needle, with its fine sharp tip, enables precise dissection and improved hemostasis during flap elevation and skin graft harvesting, thereby enhancing surgical efficiency. In this study, we report the use of the Colorado needle for harvesting a full-thickness skin graft in a patient with electric burn injury to the hand. The graft was raised with meticulous microdissection, and postoperative outcomes showed no graft loss, necrosis, or donor-site complications.
Colorado needle, electric burns, skin grafting, FTSG
Electric burn injuries represent a unique subset of thermal injuries characterized by extensive tissue destruction, often disproportionate to the size of the external wound. The hand is most frequently involved, as it is the usual point of contact with the electrical source. These injuries can lead to devastating functional and aesthetic deficits due to deep muscle, tendon, neurovascular, and bone involvement. Management requires a meticulous, staged approach involving resuscitation, serial debridement, and timely reconstruction to preserve hand function and appearance.
Reconstructive strategies for electrical burns depend on the extent and depth of tissue loss. Small superficial defects may be managed with skin grafts, while deeper or composite defects require local, regional, or free flaps. Full-thickness skin grafts (FTSGs) are preferred in certain cases for their superior durability, texture match, and minimal secondary contraction, especially over exposed tendons and joints. However, harvesting a uniform, viable full-thickness graft demands precision and hemostatic control to prevent graft loss or donor-site morbidity.
The Colorado microdissection needle is a fine-tipped electrocautery instrument designed to provide sharp, precise cutting with minimal lateral thermal damage. It allows meticulous dissection of skin and soft tissue planes with excellent hemostasis, thereby improving visibility and reducing operative time. Its use in aesthetic and reconstructive surgery has been associated with reduced intraoperative blood loss, better wound healing, and finer scar quality compared with conventional scalpels or standard cautery. [1,2]
In this case report, we describe the use of the Colorado microdissection needle in raising a full-thickness skin graft for reconstruction of a post-electric burn hand defect. The emphasis is placed on its technical advantages, safety profile, and contribution to improved surgical efficiency and outcomes.
The study was conducted in the department of Plastic Surgery in a tertiary care hospital. Informed consent was obtained from the patient after explaining the nature of the study. The study is a non-randomised prospective study. The patient was a 73-year-old male, known hypertensive and psoriatic patient. He was admitted following electric burns to the right hand leading to necrosis and wound over the thumb, middle and ring finger. Wound debridement was done followed by regular dressing and wound care (figure 1). Initially wound bed was prepared with regenerative therapies like low level laser therapy, autologous platelet rich plasma, Centenella extract, prolotherapy, collagen scaffold dressing and cyclical Negative Pressure Wound Therapy. After regenerative therapies skin grafting was done. The full thickness graft was taken done using Colorado needle for raising the graft. (Figure 2) The Colorado needle is available in various sizes with different angulation (N-series, E113-series, E103-series, E117-series, E1400-series) [3] and costs around 1500 Indian rupees.

Figure 1.Raw area over the right hand
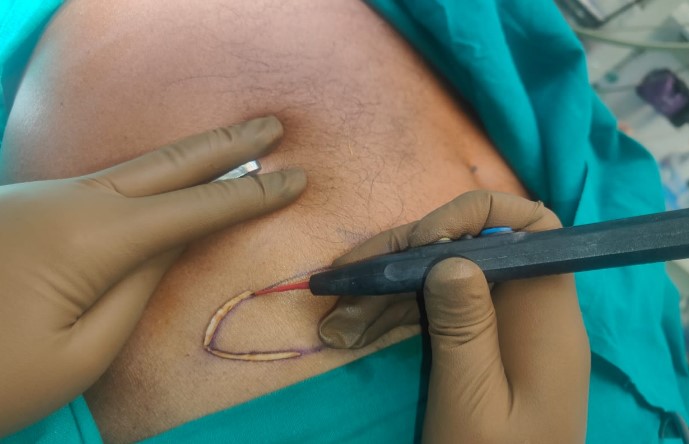
Figure 2.Colorado assisted full thickness skin graft harvest
After meticulous graft dissection with Colorado needle cautery tip no complication noted in the post operative period at both donor and recipient site (Figure 3,4). No graft loss or necrosis observed after 5 days.

Figure 3.Recipient site for the graft

Figure 4.Donor site of graft
Incisional blood loss with Colorado needle is reportedly significantly less when compared to the steel scalpel incisions. Sheikh B reported approximately four times more blood loss with a steel scalpel when compared to the Colorado micro dissection needle for scalp incisions in neurosurgical procedures. [4,5] N Nitta et al. reported that, the blood loss was three to five time lesser using the micro needle electrocautery scalpel compared to cold steel (scalpel) for scalp incisions in neurosurgical procedures. The study reported by Kearns et al, incisional blood loss with electrosurgical incisions is reportedly significantly less when compared to the steel scalpel incisions. Milan et al study showed that almost all cases had less incisional blood loss with Colorado micro dissection needle, supported by a statistically significant result. [6,7]
Perkins J determined micro dissection needle for tonsillectomy resulted decreased postoperative pain when compared with standard electrocautery. In Milan et al study, as expected, the mean pain scores for both modalities decreased at each pain assessment after surgery. The mean pain scores for Colorado micro dissection needle were less and P-value suggest statistically significant. [8,9] One of the concerns regarding electrosurgery was the theoretical risk of increased wound complications due to the heat production which results in a zone of tissue necrosis adjacent to the incision. It was proven by several studies that electrosurgically created incisions showed less increased incidence of wound complications such as dehiscence and infection. [10]
According to Milan et al study, at 6 months follow up the level of the scar as compared with surrounding skin, color match, consistency and width were normal in all the cases. N Nitta et al. suggest use of Colorado micro dissection needle, results in minimal wound damage, minimal scarring, excellent healing and minimal alopecia as it works with minimal electric contact technique. It was noted that, a Colorado micro dissection needle gives less width and better scar than cold steel (Scalpel). [11,12] There was significant less incisional blood loss intra operative and less pain post operatively compared with a cold steel (scalpel). There was no evidence of any scar tenderness or keloid formation in follow up of the cases and it was noted that, the width of post-operative scar when using Colorado micro dissection needle is lesser and better healing than cold steel (Scalpel). Also, the time taken for incision with Colorado micro dissection needle was lesser than cold steel, but it was statistically insignificant.
The Colorado micro dissection needle is both safe and useful in surgical procedures compared to other modalities.
Conflicts of interest:None
Authors’ contributions:All authors made contributions to the article
Availability of data and materials:Not applicable.
Financial support and sponsorshipNone.
Consent for publication:Not applicable