Dr Sandesh Thete*
1Associate professor, Malati Multispeciality Hospital and Medical College, Turkhed, Akola, Maharashtra
*Correspondence: Dr Sandesh Thete, Associate professor, Malati Multispeciality Hospital and Medical College, Turkhed, Akola, Maharashtra, E-mail: sandeshthete1985@gmail.com
Received date: 02 April, 2026; Accepted date: 22 April, 2026; Published date: 28 April, 2026
Citation: Sandesh Thete. “Diagnostic Role of MRI in Early Detection of Osteolysis Following Total Knee Arthroplasty.” J Healthc Adv Nur (2026): 136. DOI: 10.59462/3068-1758.4.1.136
Copyright: © 2026 Sandesh Thete. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Recovery from bipolar disorder is not typically considered a possible outcome within psychiatry. This article presents an autobiographical clinical case of bipolar disorder that began in adolescence and continued for approximately 33 years. In subsequent years, after serious psychological work, depressive and manic phases completely ceased. The author considers this condition as recovery and analyzes the possible mechanisms of these changes within the biopsychosocial model (Engel, 1977). Particular attention is given to distinguishing two levels of intervention: the biological and the psychological, with an emphasis on how the inner work led to a structural reorganization of personality. Based on personal experience, the author proposes criteria for differentiating between remission and recovery and raises the question of the need to reconsider the prevailing view of bipolar disorder as a lifelong chronic illness.
Keywords: Total Knee Arthroplasty, Osteolysis, MRI
Total Knee Replacement (TKR) has become a successful procedure for the relief of pain, correction of deformity, and restoration of function in arthritic knees in elderly patients [1]. Advances in technology and design have enabled more predictable results and these advances, together with the creation of longer-lasting materials [2] have made TKR both a predictable and a durable procedure in the elderly.
Total Knee Arthroplasty (TKA) is a very successful reproducible procedure and an excellent treatment in eliminating pain and restores function in a diseased knee for both the short term and long-term period. However, osteolysis remains a problem in long term follow up cases of TKA. Osteolysis secondary to polyethylene wear and particulate debris has been recognised as a cause of periprosthetic bone loss around Total Knee Arthroplasty [3-4].
The presence and magnitude of periprosthetic bone loss is important to assess because it determines when operative treatment is indicated and anticipated and also for improved preoperative planning.
Osteolysis around TKA can be difficult to identify and quantitate on plain radiographs especially osteolysis behind the femoral component [5].
As the fixation of total joint implants has become more reliable and durable and as the technology of total joint replacement has been applied to younger and more active patients, the current limitations of total joint arthroplasty are related to the wear of the components [6].
Wear is the removal of material, with the generation of wear particles that occurs as a result of the relative motion between two opposing surfaces under load. In complex mechanical-biological systems such as total knee replacements, there can be many types of wear. Although the mechanical consequences of wear, such as progressive thinning of polyethylene components, can limit the functional life of a joint replacement, the clinical problems from wear more frequently are due to the release of an excessive number of wear particles into a biological environment. When particles within a certain size-range are phagocytised in sufficient amounts, the macrophages enter into an activated state of metabolism, releasing substances that can result in periprosthetic bone resorption. Progressive loss of periprosthetic bone can necessitate a reoperation, which is the definitive measure of clinical failure of a joint arthroplasty.
Clinical symptoms, plain radiograph, and Computed Tomography (CT) scan have been used to study the extent and the natural history of osteolysis. Early on in the disease process, patients may be asymptomatic. Most patients, however, will present with symptoms of pain, swelling, and acute synovitis with or without osteolysis on radiographs. Serial radiographs are then necessary to evaluate its progression. The rate may depend on the patient's age, sex, host response, activity level, alignment, and stability, type of polyethylene, locking mechanism, fixation method, and duration of implantation.
The average time until the radiographic appearance of osteolysis is around 31 months. [7] In most cases, progressive bone resorption due to osteolysis leads to femoral component loosening [8]. Loss of bone support from osteolysis also leads to weakness in the periprosthetic area and abnormal stress concentration about the implant, resulting in periprosthetic fractures and acute pain, or even component fracture [9].
The identification of osteolysis on plain radiographs can be difficult:
It has been estimated that 50% of the skeletal calcium must be lost before a change can be seen on the radiograph.
The femoral and tibial components may block visualization of the cancellous bone adjacent to the prosthesis.
Nadaud [5] recommended oblique radiographs to evaluate femoral bone stock. In general, radiographs underestimate the amount of osteolysis seen intraoperatively. Whereas CT scanning is the more popular radiological study to assess the extent of osteolysis, recent evidence suggests that magnetic resonance imaging (MRI) is a more sensitive method. The sensitivity of detecting lesions by MRI was 95.4% as compared to 74.7% with optimized CT scan and 51.7% with plain radiography, including bilateral oblique views [10].
Magnetic resonance imaging has the added advantage of showing the granulomatous tissue caused by the wear particles, as well as capturing intracapsular synovial disease before discernible bone loss. The role of MRI in the early detection of wear, osteolysis, and fixation failure warrants further investigation.
In this retrospective study we use MRI with metal suppression for evaluation of osteolysis around Total Knee Arthroplasty and correlate these findings with plain radiographs and use this information for facilitation of preoperative discussion with the patient as well as pre-operative planning [11].
To evaluate early osteolysis around Total Knee Arthroplasty patients who have undergone Total Knee Arthroplasty more than five years before, using MRI with metal suppression.
Osteolysis around Total Knee Arthroplasty have so far been studied using plain radiographs. This has frequently led to under estimation of bone loss. We are using three-dimensional imaging modalities like MRI with metal suppression for evaluation of osteolysis in more than five-year post-operative follow up Total Knee Arthroplasty and correlate these findings with plain radiographs.
Studies so far show encouraging results with MRI.
Thus, by evaluating more than five-year post-operative Total Knee Arthroplasty using MRI with metal suppression we intend to identify and determine:
The extent of early osteolysis that is X-Ray negative phase.
The extent of osteolysis in X Ray positive patients and correlating these findings with MRI.
This information thus can be used for early reparative measure to prevent ultimate failure of total knee implant.
Course of the Illness
The illness began in adolescence with a depressive episode and continued for approximately 33 years, manifesting in typical depressive and manic phases. Depressive states lasted for months and were accompanied by pronounced symptoms: feelings of guilt, delusions of shame, loss of concentration and memory, sleep disturbances, complete loss of appetite, and significant weight loss. During this period, there were suicide attempts.
Manic phases were characterized by accelerated thinking, an intense flow of ideas, a combination of euphoria and irritability, and severe insomnia. Sleep became increasingly shorter regardless of bedtime and was unresponsive to intervention. Behavior during this period became impulsive and unpredictable, although no dangerous actions towards others occurred.
Treatment was conducted within the conditions of Soviet psychiatry and included intensive therapeutic methods: insulin coma therapy, sulphazine, and aminazine. The first manic episode occurred during hospitalization. Despite the long course of the illness, the author continued to work and maintained professional activity throughout her life, except during periods of hospitalization.
Osteolysis
Peter’s et al defined osteolysis as identification of a lytic osseous defect that extends beyond the limits of that potentially caused by loosening of the implant alone, absence of cancellous-bone trabeculae, and geographic demarcation by a shell of bone [12].
Osteolysis is one of the leading causes for late reoperation in patients who undergo total knee arthroplasty (TKA). Five years after primary TKA, the number one cause of revision is osteolysis due to polyethylene wear [13]. Osteolysis has been noted with both cemented and cementless modular total knees, ranging between 6% and 30% for cementless TKA and between 0% and 16% for cemented TKA.
The earliest report of osteolysis after TKA was in 1992, when Peters [12] found a 16% rate of osteolysis 1 to 5 years after 176 cementless TKA were implanted with screw fixation. Holes in the tibial base plate, tibial fixation screws, and areas of unbonded or discontinuous porous coating on the implants were implicated as the conduits for debris leading to osteolysis [14]. In 1994 to 1995, osteolysis was also noted when components were inserted with cement [15] In these instances, debris was believed to gain access to the metaphyseal bone by way of voids in the cement mantle or by direct invasion of the metaphyseal bone by histiocyte-laden synovial tissue.
Etiology
Osteolysis occurs as the result of a foreign body response to particulate wear debris from the prosthetic joint. These particles consist of polyethylene, polymethylmethacrylate cement, and metal, all of which have been shown to elicit a distinct inflammatory response [16]. The particle's size, shape, type, and concentration are major determinants of its bio reactivity.
The incidence and extent of osteolysis after TKA are less than that after Total Hip Arthroplasty (THA). In TKA, the predominant mode of failure is due to fatigue, which produces polyethylene particles that are larger and more irregular in shape when compared with those after THA, in which the predominant mode of failure is abrasive and adhesive wear.
In an analysis of wear particulate debris retrieved from 18 failed TKA showed that the mean particle size was 1.7 ± 0.7 μm or an average of 3 times larger than particles in THA [17]. Smaller-sized particles have an increased biological activity, resulting in an increased rate of osteolysis after THA.
Horikoshi [18], who performed biochemical and histological analyses of the interface membranes in 16 knee implants found significantly smaller particles in the membranes from failed THA, which had a higher activity of stromelysin, prostaglandin E2, interleukin-1 (IL-1), and tumor necrosis factor.
Once the particles are generated from and around the implant, they become phagocytised by macrophages and giant cells in the synovial or periprosthetic tissue. These cells, in turn, become activated and can directly or indirectly cause osteolysis. Direct osteolysis was observed by [19]. His findings showed that foreign body–induced macrophages were capable of direct low-grade bone resorption. However, indirect osteolysis is more common. Once the synovial or periprosthetic macrophage is stimulated, cytokine production is activated. Interleukin-1β is one of the many cytokines released by these activated macrophages, which is pro-inflammatory and causes osteoclastic stimulation. Interleukins are present in significantly higher concentrations in knees having revision surgery than in osteoarthritic knees, reflecting a greater inflammatory response in the former [20]. Cytokines also cause decreased bone formation by osteoblasts [11].
The type of metal particles also has a significant effect on the extent of osteolysis. Titanium has a greater stimulatory effect than Chromium-Cobalt (CrCo) in releasing IL-1β. Haynes [19] described that CrCo particles cause early death of the macrophages, diminishing the inflammatory mediators implicated in osteolysis, whereas titanium particles were minimally toxic to the macrophage, thereby triggering higher levels of inflammatory mediation.
The activated osteoclast is the primary cell responsible for the osteolytic response occurring in TKA. Osteoclastic activity and, hence, osteolytic rates can be monitored using Tartarate Resistance Acid Phosphatase (TRAP) levels in synovial aspirates [22]. Kovacik [20] showed a higher level of TRAP in knees undergoing revision surgery than in knees undergoing primary TKA.
Osteolysis can occur anywhere around a TKA, although it is common in certain anatomic regions. The femur is prone to osteolysis in the region of the femoral condyles and near the attachments of the collateral ligaments of the femur. It is unknown why these regions are so susceptible to osteolysis, although hydrostatic pressure and soft cancellous bone have been postulated. Osteolysis around the tibia tends to occur along the periphery of the component or long the access channels to the cancellous bone.
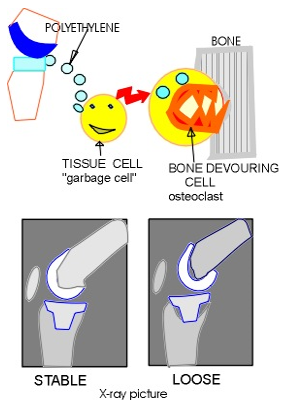
Figure 1: Mechanism of Osteolysis
Diagnosis
Clinical Symptoms
Plain Radiograph
Computed Tomography (CT) scan
Magnetic Resonance Imaging (MRI)
have been used to study the extent and the natural history of osteolysis. Early on in the disease process, patients may be asymptomatic. Most patients, however, will present with symptoms of pain, swelling, and acute synovitis with or without osteolysis on radiographs. Serial radiographs are then necessary to evaluate its progression. The rate may depend on the patient's age, sex, host response, activity level, alignment, and stability, type of polyethylene, locking mechanism, fixation method, and duration of implantation. The average time until the radiographic appearance of osteolysis is around 31 months [7].
In most cases, progressive bone resorption due to osteolysis leads to femoral component loosening [8]. Loss of bone support from osteolysis also leads to weakness in the periprosthetic area and abnormal stress concentration about the implant, resulting in periprosthetic fractures and acute pain, or even component fracture.
The identification of osteolysis on plain radiographs can be difficult. First, it has been estimated that 50% of the skeletal calcium must be lost before a change can be seen on the radiograph [11]. Second, the femoral and tibial components may block visualization of the cancellous bone adjacent to the prosthesis.
Lonner [26] reported a 22% incidence of osteolytic defects at the time of revision surgery, whereas the prerevision radiographs showed lesions in only 4% of these cases. Nadaud [5] recommended oblique radiographs to evaluate femoral bone stock. In general, radiographs underestimate the amount of osteolysis seen intraoperatively.
Whereas CT scanning is the more popular radiological study to assess the extent of osteolysis, recent evidence suggests that Magnetic Resonance Imaging (MRI) is a more sensitive method. The sensitivity of detecting lesions by MRI was 95.4% as compared to 74.7% with optimized CT scan and 51.7% with plain radiography, including bilateral oblique views [5].
Magnetic resonance imaging has the added advantage of showing the granulomatous tissue caused by the wear particles, as well as capturing intracapsular synovial disease before discernible bone loss. The role of MRI in the early detection of wear, osteolysis, and fixation failure warrants further investigation [27].
Factors affecting polyethylene wear:
Although a reliable method for measuring polyethylene wear in THA in radiostereometric analysis is well established, no method currently exists for measuring wear in TKA. The complex geometry of the femoral and tibial components makes the radiographic measurement of wear difficult and inaccurate. Moreover, the larger particles produced by delamination do not cause osteolysis. Therefore, even if wear in TKA could be accurately measured, a correlation may not exist between radiographically determined wear and osteolysis.
The most precise method of measuring wear in TKA is a computerized technique that uses a single plane radiograph and a 3-dimensional/2-dimensional matching algorithm to determine the 3-dimensional position and orientation of each knee implant. The distance from the femoral component to the tibial component is then measured to determine the amount of wear. Using this technique, the root mean square error was reported to be as low as 0.04 mm [11].
Topside Wear
Wear particles generated at the topside, or the primary articulating surface, are caused by pitting and surface delamination. Although this is the dominant damage mechanism after TKA, adhesive and abrasive wear also exist. Delamination is the primary cause of most polyethylene-related total knee failures. The process occurs due to the initiation and propagation of subsurface cracks and can result in the removal of large (>0.5 mm) flakes of polyethylene.
Modularity
The weak link in most modular components appears to be the locking mechanism by allowing motion between the polyethylene insert and the metal base plate. This motion may increase after a period of in vivo loading. This was first reported by Engh, who measured the AP and mediolateral motion between the polyethylene insert and the tibial tray in a variety of modular total knee tibial components and showed increased motion over time.
Backside Wear
Micro motion between the tibial tray and the polyethylene resulting in backside wear has emerged as a new player in the source of particles causing osteolysis. Recent reports have demonstrated that the wear at the under surface of the tibial insert of modular components may be more severe than originally believed.
Resin Type
The type of polyethylene and its sterilization method can have substantial effects on the long-term performance and the incidence of osteolysis. There are currently 2 resins that can be selected for poly inserts, GUR 1020 and GUR 1050. These are powder forms supplied by Ticona and later converted into a bulk solid form by secondary processors via either ram extrusion, compression molded sheets, or direct compression moulding.
There is no comparative clinical study that demonstrates a clear clinical advantage to either resin species or manufacturing method. Furthermore, there are no clinical studies that directly compare the various materials with a single implant design in a properly designed study.
Quality of Polyethylene
The quality of polyethylene supplied by different vendors at different times may vary. Moreover, processing defects can result in subsurface cracks, voids, or fusion defects. These imperfections can act as sites for delamination or further crack propagation when loaded in vivo.
Sterilization
The methods of sterilization have a major effect on the wear characteristics of a polyethylene. There continues to be debate over the best methods for sterilization of the polyethylene components. At present, there are 2 types of sterilization used, gamma irradiation and chemical sterilization. In the chemical sterilization category, both gas plasma and ethylene oxide gas are used. In a retrospective study, Williams compared 1603 polyethylene components that had been sterilized with gamma irradiation in air and retrieved after an average of 57 months in vivo with 32 components that had been sterilized with ethylene oxide gas and retrieved after an average of 115 months in vivo. Fifty-five percent of the components in the former group showed evidence of delamination, whereas none of those in the latter group appeared to have delamination-type damage.
Polyethylene Thickness
Polyethylene thickness is a major determinant for its wear properties. Bartel [28] has shown that the contact stresses in polyethylene increase exponentially as thickness of the implant decreases. They concluded that a thickness of more than 8 mm of polyethylene should be used in clinical practice. Clinical reports of retrieved implants subsequently affirmed this theory.
Bearing Surface Conformity
Bartel et al have shown that the effect of contact load and stress distribution at the bearing surface is dependent on the surface area over which weight-bearing stresses are transferred [28]. Bearing surface designs with poorly conforming femoro-tibial contact areas have high stress level in the polyethylene. These types of articulations attempt to reproduce physiologic movements in the knee by allowing motion to be dictated by the soft tissues and ligamentous structures, particularly the posterior cruciate ligament [8]. Highly congruent articulation design maximizes contact area and wear resistance but may decrease the load carried by the surrounding soft tissues and subsequently increase stresses at the component-bone interface.
Surface Roughness
Surface roughness of the femoral component plays a role in causing abrasive wear of the polyethylene. Puloski [29] The major difference was noticed in the cam that was uniformly rougher than the condylar surface or the trochlea in 6 of the 9 components. This study emphasized that the additional interface of the cam post mechanism is a potential source of wear debris, and surface roughness of this articulation needs to be optimized during manufacturing.
Shelf Life
Shelf life is one of the most important variables affecting the wear properties of polyethylene. Fehring [30] showed that for each year increase in shelf age, the hazard of having wear-related failure increased by 187%.
Fixation Methods
Attempts to decrease the rate of osteolysis have been made by optimizing bone ingrowths into cementless porous surface implants. Nevertheless, osteolysis rates with cementless fixation have been reported to be as high as or higher than those rates with cemented fixation. However, in these reports, it is difficult to relate the osteolysis solely to the method of fixation because causes of polyethylene wear are multifactorial.
Age and Sex
Age and sex have an impact on the rate of osteolysis after TKA.
Fehring [30] in a study of 2091 PFC implants showed that for each 1-year decrease in patient age, the likelihood of having wear-related failure increased by nearly 5%. This could be due to the increased activity level of younger patients as shown in a pedometer study reported by Schmalzried, who found that patients younger than 60 years walked 30% more than those who were 60 years and older.
Those studies reported that men are 2.8 times more likely to have a wear-related failure than women, which may be due to a 28% increased activity by men in comparison to women.
Rotating Platform Implants
Current TKA designs can be subdivided into 2 fundamental principles: Fixed Bearing (FB) knees, where the polyethylene insert press fits into the tibial tray, and rotating-platform (RP) designs, which allow for rotation of the insert relative to the tray. Rotating-platform knees have been shown to significantly reduce volumetric wear [31].
Treatment
The current literature does not support any fixed algorithm for the management of osteolysis in TKA at its various stages. The patient is asymptomatic with minimal osteolysis on plain radiographs, regular follow-up at 6 months to 1 year with medical management to include calcium and bisphosphonates is recommended. MRI to define the size and location of the osteolysis is very helpful in managing these patients. If the patient becomes symptomatic or the osteolysis is progressive, then early liner exchange with or without tibial base plate exchange is considered.
If the patient with established osteolysis presents with acute pain, one should rule out acute metaphyseal fracture versus infection. Fractures will often heal with protected weight bearing, at which point revision surgery can be contemplated if necessary. At revision surgery, if the metaphyseal bone stock is adequate, hybrid fixation for the femoral and tibial stem is our recommendation. If the metaphysis is eroded, then the femoral and tibial condyles can be reconstructed with an allograft and protected by fully cementing the stem.
Future Improvements/Issues
Recent changes to current TKA designs have focused on reducing backside wear by improving polyethylene, improving locking mechanism tolerances to less than 50 μm, using polished CrCo base plates, using RP designs, and returning to one-piece tibial units either metal-backed or all-polyethylene.
Highly cross-linked polyethylene (XPE) has been shown to reduce wear in THA; however, its applications in TKA are just emerging. In a multidirectional pin-on-plate wear study of non–cross-linked, moderately cross-linked (5 Mrad), and highly cross-linked (10 Mrad) polyethylene showed a 75% reduction in wear with the highly cross-linked material under hip kinematics, but only a 33% reduction wear in knee kinematics. Moreover, he also performed direct cell culture studies of wear debris generated in sterile wear stimulators, which showed an increase in tumor necrosis factor-alpha levels and reactivity for GUR 1050 highly cross-linked polyethylene debris compared with an equivalent volume of non–cross-linked GUR 1050 polyethylene. Hence, although XPE causes decreased wear, the smaller nature and high bio reactivity of these particles may cause an increased rate of osteolysis. The in vivo benefits of XPE will become more evident with longer-term clinical follow-up. The future material developments in XPE will be the addition of antioxidants such as vitamin E to limit the amount of in vivo oxidation.
Other strategies to reduce wear in general have focused on alternative bearing materials. Among these bearings, ceramic-polyethylene has some theoretical advantages over metal-polyethylene, including its thermodynamic and chemical inertness, high wettability, low coefficient of friction, and high resistance to damage by third body wear. Alumina ceramics has been available for THA since 1970. Recent improvements in ceramic quality have allowed the manufacture of more complex implants, including femoral and tibial components for TKA. One such implant is Kyoto total knee cementless prosthesis (KC-1), (Yokohoma Medical Ceramic Knee type, Kyocera, Kyoto, Japan). Its femoral component is made of alumina ceramics that articulates with an XPE plate supported by a ceramic tibial plate. However, Tateishi [32] in 1993 reported on 23 patients with rheumatoid arthritis with KC-1 prosthesis in situ, of which 6 knees had to be revised because of failure of fixation of tibia base plate.
Zirconium is a metal, which when oxidized becomes a ceramic, Zirconia. Components are now available, which are manufactured with a metal zirconium core and a ceramic zirconia-articulating surface. These components are manufactured through oxygen diffusion of the substrate in a high heat environment, which allows a transformation of the surface of the implant from metal to ceramic. The resulting material maintains the strength of the metal zirconium core, yet provides the benefit of a ceramic-articulating surface. Ezzet [33] measured the wear in 3 sets of non–cross-linked ultrahigh molecular weight polyethylene against oxidized zirconium femoral components (Profix TKA, Smith & Nephew, Memphis, Tenn) and Co-Cr femoral components of identical geometry in a knee wear stimulator. Oxidized zirconium reduced polyethylene wear by 42% compared with Co-Cr alloy.
Laskin [34] observed no adverse effects clinically or radiologically at 2-year follow-up of 76 patients with the Genesis II prosthesis with an Oxinium oxidized zirconium femoral component. Concerns have been raised, however, with regard to the thin layer (less than 5 μm) of this coating and its potential for easy surface damage.
Although it is our hope that these design changes will have a positive impact on the reduction of wear and the development of osteolysis, only time will tell. Long-term, clinical follow-up is desperately needed to establish any new benchmarks. Many changes made in the past have had untoward or unexpected outcomes. This may be especially true of the recent trend toward high flexion designs. Nonetheless, progress marches on. Finally, it cannot be overemphasized that wear and osteolysis after TKA are late complications. Early failure as a result of loosening, instability, malalignment, and infection is still a looming problem secondary to improper surgical technique.
Imaging in Osteolysis:
The earliest report of osteolysis after TKA was in 1992, when Peters [12] had defined osteolysis as identification of a lytic osseous defect that extends beyond the limits of that potentially caused by loosening of the implant alone, absence of cancellous-bone trabeculae, and geographic demarcation by a shell of bone.
Naudie [5] suggested that wear of any of the components of a knee replacement (Polyethylene, Metal, Methylmethacrylate Cement) will cause shedding of particles which may incite a histiocytic response which in turn leads to osteolysis, but polyethylene wear is the most common cause.
Berry [3] showed that osteolysis will occur wherever the histiocytes have access; thus, if a component is already loose, osteolysis will occur at the interfaces of that component, while in the well-fixed arthroplasty, histocytic osteolysis occurs in the posterior aspects of the femoral condyles and the condylar attachments of the collateral ligaments, around the periphery of the tibial base plate and along the stem or any screw holes, and at the patellar component interface or around the margin of the patellar component
Knees with a particle-induced histiocytic response typically have joint effusions due to synovitis [6], and the effusion contains interleukin—1 beta and tartarate resistant acid phosphatase, which are not found in non-osteolytic conditions [10].
Fehring [7] showed both cemented and non-cemented tibial components normally may develop a thin (<1 mm) lucency around the base plate and stem [7]. Interval increase in width of the lucency, the development of focal radiolucency’s greater than 2 mm, and component migration are abnormal and indicate loosening, but the distinction between aseptic loosening (due to mechanical loosening or histiocytic response) and septic loosening usually cannot be made radiographically.
X Rays:
AP
Lateral
Sunrise or merchant radiographs
Oblique posterior condylar view
Are the radiographic views as advocated?
Periprosthetic lucency may be underestimated if the X-ray beam is not perfectly tangential to the component-bone interfaces and osteolysis may be obscured by the components themselves [10].
Advocate the use of fluoroscopically-guided radiographs to obtain true tangential radiographs,
Naudad [5] suggest an oblique posterior condylar view in order to better visualize radiolucencies around the posterior aspects of the prosthetic condyles that were otherwise obscured on conventional lateral radiographs.
Lonner showed lucency beneath the tibial base plate can also occur due to a phenomenon called “stress shielding”. Bone requires a phyiologic load in order to stay dense; if the tibial component has a long stem with distal fixation, the tibial base plate will no longer transmit load to the underlying bone, thus shielding it from stress, and the bone may become osteopenic and thus subject to fracture.
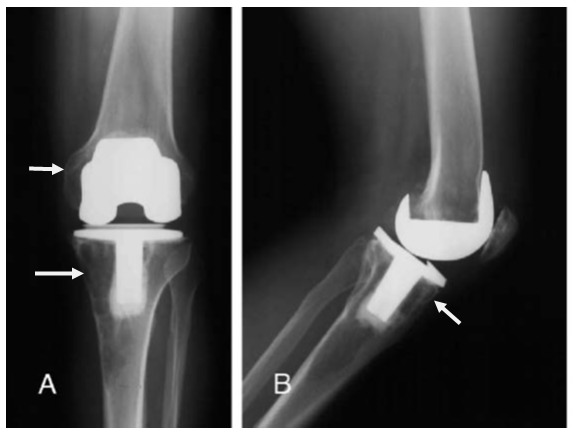
Figure 2: Plain Radiograph (Ap And Lat View)-Showing Osteolysis
CT Scan:
Puri [34] advocated the use of CT to detect osteolysis. When applied with a multidetector, helical CT at a higher kilovolt peak (140 kVp) improves penetration by the x-ray and results in superior image quality, with superior sensitivity compared with conventional radiographs). These techniques also increase the effective dose, which can prove a burden for serial CT evaluations.
MRI:
MRI consistently quantified better the extent and location of osteolysis compared with radiographs [13]. MRI to detect intracapsular deposits before the osteoclastic resorption of bone. The ability to detect intracapsular synovial deposits may prove helpful in the longitudinal assessment of osteolysis, gaining more sensitive detection of early particle disease in patients presenting with painful arthroplasty despite the presence of normal radiographs and no MRI evidence of bone loss. The ability of MRI to quantify synovial deposits also may prove useful in the evaluation of nonoperative treatment modalities, such as the use of oral bisphosphonates.
In the setting of massive osteolysis, plain radiographs are typically positive. MRI in this setting may be useful not only in detecting adjacent compromise of neurovascular structures, but also in the more precise quantification of bone loss,
providing appropriate guidance with regards to bone graft requirements and sizing of components. The presence of component loosening is typically manifest as circumferential increased signal intensity between the metallic-bone or cement bone Interface. CT detected 65 of 87 lesions, resulting in a specificity of 75%, with greater sensitivity for CT and radiographs in the ilium, with relatively poor depiction in the anterior column and pubis [13]. In contrast, MRI consistently had good lesion detection regardless of location and correctly identified 83 of 87 possible lesions, yielding a sensitivity of 95%. Specificities were equivalent, with all techniques showing relatively high specificity (96–100%). These data indicate the superior
ability of MRI to detect bone loss.
Radiographs remain, however, a 2-dimensional assessment of a 3-dimensional disease process, and studies have shown that they grossly underestimate the extent of osteolysis, with limited sensitivity [12, 34] and poor interobserver reliability [34] Although computed tomography (CT) more precisely quantifies osteolysis as compared with radiographs, reduction of the beam-hardening artifact requires an increase in ionizing radiation exposure, especially as serial studies are often needed [12, 13]. In addition, neither CT nor radiographs are capable of identifying early intracapsular particle wear, which is thought to exist before bony resorption, and they are both of limited value for the visualization of soft-tissue pathology localized in the periprosthetic envelope.
More recently [24] had studied the use of MRI with metal suppression for detection of osteolysis. MRI with metal suppression provides better information, in specific instances, to help determine appropriate candidates for surgical intervention or clinical observation. Focused primarily on the value of MRI to assess osteolysis
around TKA.
[13] studied MRI after TKA in 41 patients (46 knees) with particular emphasis on the evaluation of periprosthetic soft tissues. That study demonstrated
that MRI with metal artefact suppression was effective in yielding diagnostic information about knee arthroplasty.
A recent study of 28 hip arthroplasties by Potter et al demonstrated good
association between MRI and plain radiographs in determining the presence and extent of osteolysis [13].
Given its multiplanar capabilities, lack of ionizing radiation, and superior soft-tissue contrast, magnetic resonance imaging (MRI) offers significant potential advantages for evaluating the joint after arthroplasty.
Although traditional MRI techniques are limited by the presence of artefact generated by the metallic components, recent refinement and modifications of pulse sequences have allowed for the evaluation of the bone-implant interface and the surrounding soft tissues due to reduction of susceptibility artefact [13].
In this study we intend to see the usefulness of MRI in detecting early osteolysis and quantify it fairly accurately in five years or more post-operative TKA patients.
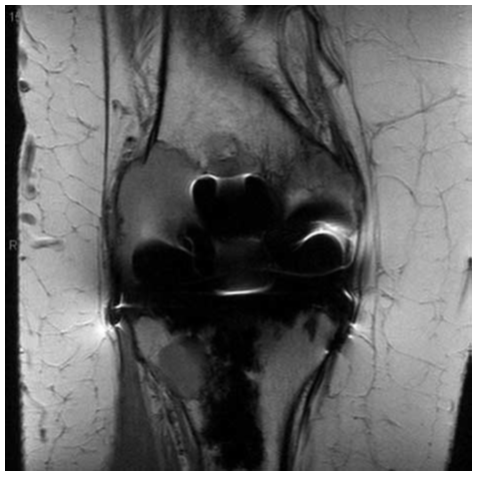
Figure 3: Turbo spin-echo pd-weighted coronal image of right knee of patient 2, demonstrating a large area of osteolysis of the lateral and medial condyles of the femur and in the proximal lateral tibia.
Materials and Methods
This retrospective review included 22 primary TKA knees who had undergone TKA more than 5 years before. All were referred for MRI with metal suppression after clinical evaluation and plain radiographs, to determine either the extent or presence of suspected periprosthetic osteolysis.
During the study period, 22 knees were referred for evaluation of their knee arthroplasty with MRI with metal suppression. There were 3 men and19 women with a mean age of 67 years (range, 55-80 years). The diagnosis leading to the primary knee arthroplasty was osteoarthritis, one patient had posttraumatic arthritis.
Mean length of time in situ for the arthroplasties was 6 years (range, 5-7 years). MRI included all posterior cruciate ligament–substituting prostheses. All components were fixed with cement.
All plain radiographs were reviewed by 2 independent authors, who at the time of review, were blinded as to patient identity and clinical outcome. These radiographs included weight-bearing anteroposterior, lateral, and oblique views.
Periprosthetic osteolysis was defined as identification of a lytic osseous defect that extends beyond the limits of that potentially caused by loosening of the implant alone, absence of cancellous-bone trabeculae, and geographic demarcation by a shell of bone.
The size of the lesions was obtained by measuring the longest diameter in one dimension and the longest dimension orthogonal to the first on anteroposterior and lateral radiographs.
For all lesions (femoral, tibial, and patellar), an attempt was made to measure in these dimensions, that is,
Longest diameter in one plain
Longest diameter in orthogonally opposite plain,
Radiographs were also evaluated for component fixation, component failure, presence of periprosthetic fracture or cortical destruction, and presence or absence of an effusion.
The MRI protocol was according to Hospital for surgery recommendations.
All images obtained centered on the joint. This protocol was performed with an MRI unit with a 1.5-T magnet and current standard software applications. (Siemens, Somatom 1.5 T)
The MRI technique used in this study differs from standard MR sequences used in routine knee imaging in several important ways.
The pulse sequences used in this study consisted of FSE T1–weighted and proton density–weighted images and FSE IR images with expanded receiver BW and ETL.
Although FSE imaging is used in standard MR imaging of the host knee in many centers, this is typically performed with a low receiver BW, that is, less than 16 MHz and typically with an ETL of 8 or less. Increasing the receiver readout BW allows for increased echo sampling which helps minimize susceptibility artefact.
Increasing the ETL shortens the time between the multiple refocusing pulses inherent to FSE imaging, thereby decreasing the amount of time available for proton dephasing and the attendant loss of signal. IR images, which yield effective
T2 weighting, are less susceptible to metallic artefact than the traditional SE or FSE T2–weighted images with chemical fat saturation as they are less sensitive to the variations in the main magnetic field induced by metallic orthopaedic hardware.
All MRI scans were reviewed by the authors, who at the time of review were blinded to patient identity and clinical outcome.
Periprosthetic osteolysis was defined as well-demarcated, intermediate to slightly increased signal intensity areas of focal marrow replacement with an additional line of low signal intensity as described by [13].
Lesion size was directly measured in 3 orthogonal planes. (AP –antero posterior,SI –superoinferior,ML-mediolateral)
MRI images were also evaluated for the presence or absence of joint effusion, the characteristics of the effusion, and the presence or absence of juxta-articular masses and signal characteristics of the said masses.
Approximate assessment of intralesional area was done on the plain radiographs and volume on MRI. Averages of the dimensions of the lesions on plain radiographs was calculated. Averages of the actual superior-to-inferior, medial to-lateral, and anterior-to-posterior measurements of each lesion on MRI were calculated.
Osteolysis was identified or suspected on plain radiographs of 6 of 22 patient knees 4 of 22 knees had osteolysis in tibia and 3 in femur. On MRI, knees showing osteolysis was 8 of 22.
Total no. of osteolytic lesions on plain radiographs were 7. (Tibia-4, Femur-3). Total no. of lesions on MRI was 11. (Tibia-7, Femur-4).
In 5 of 22 knees, the extent of osteolysis was underestimated on plain radiographs compared with MRI. In one case, osteolysis suspected on radiographs was not confirmed by MRI.
5 of 22 knees had x ray negative MRI positive osteolysis. (Tibia-3, Femur-2)
7 osteolytic lesions identified by MRI were lesions located in the proximal tibia, and 4 lesions were located in the distal femur. In overall 22 knees 2 knees were clinically symptomatic with osteolysis seen in tibia and femur detected on plain radiographs and MRI.
9 of 22 knees showed osteolysis either in tibia or femur or both. (On plain radiographs and MRI). The average duration post TKA was 7 years.
MRI also demonstrated secondary osteolytic lesions which were radiographically occult.
The average lesion dimension measured on plain radiographs were calculated as follows-
Longest diameter in one plain
Longest diameter in plain orthogonal to the first.
The lesion dimension measurement on MRI was as follows –
AP (anteroposterior)
ML (mediolateral)
SI (supero inferior)
Average lesion dimension calculated by X ray and MRI are shown in table 1.
The average area of the osteolytic lesion (in tibia and femur) calculated from plain radiographs shown in table 2.
The average volume of the osteolytic lesion (in tibia and femur) calculated from MRI shown in table 2.
All plain radiographs were reviewed by 2 independent authors, who at the time of review, were blinded as to patient identity and clinical outcome. The results are as follows:
|
|
Blind observer A |
Blind observer B |
|
TIBIA |
7 Lesions |
5 Lesions |
|
FEMUR |
7 Lesions |
4 Lesions |
|
|
X ray (mm) |
MRI (mm) |
|
TIBIA |
16 |
18.5 |
|
FEMUR |
13 |
16 |
Table 1: Average Lesion Dimension
|
|
Area of Osteolysis on X RAYS (mm2) |
Vol. of Osteolysis on MRI (mm3) |
|
TIBIA |
262 |
5109.3 |
|
FEMUR |
259 |
6478.31 |
Table 2: Quantification of Osteolysis Seen by Plain Radiographs And MRI
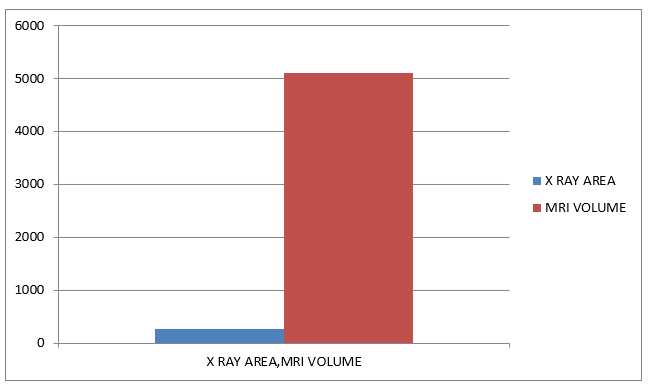
Chart 1: Comparison of radiographic area and MRI volumes of Osteolysis in Tibia
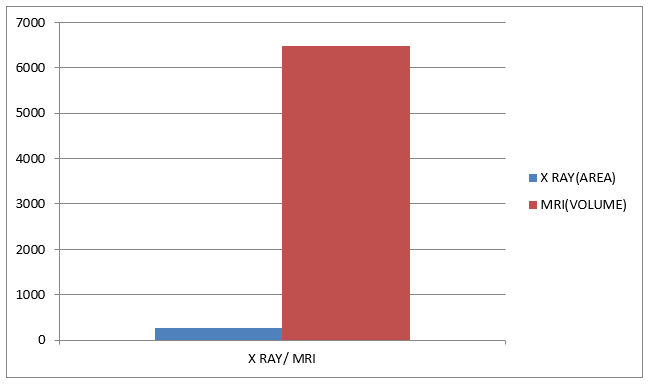
Chart 2: Comparison of radiographic area and MRI volumes of Osteolytic in Femur
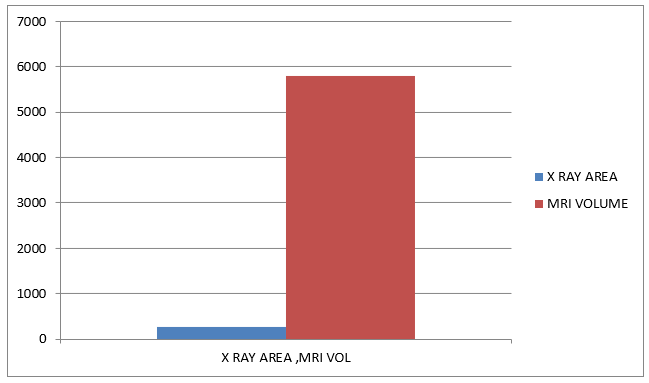
Chart 3: Comparison of Average Radiographic Area and MRI Volumes of Osteolysis
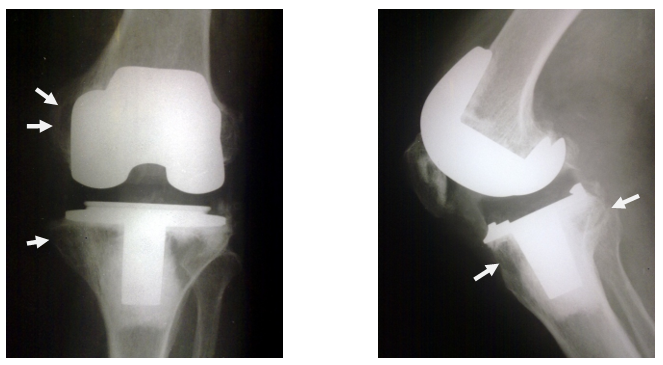
Figure 4: Plain radiograph of a patient showing Osteolysis both in Tibia and Femur (white arrows)
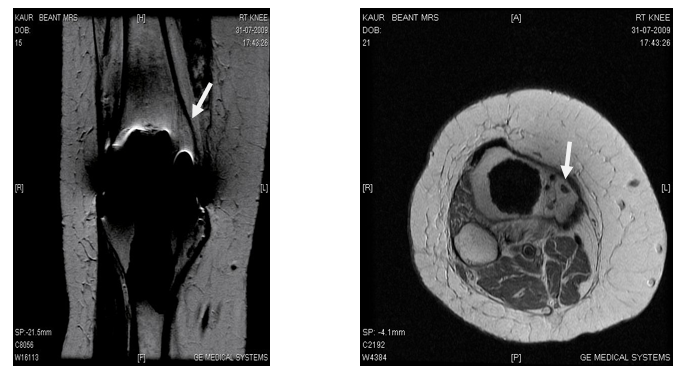
Figure 5: MRI of the same patient showing Osteolysis in Femur and Tibia of significant amount
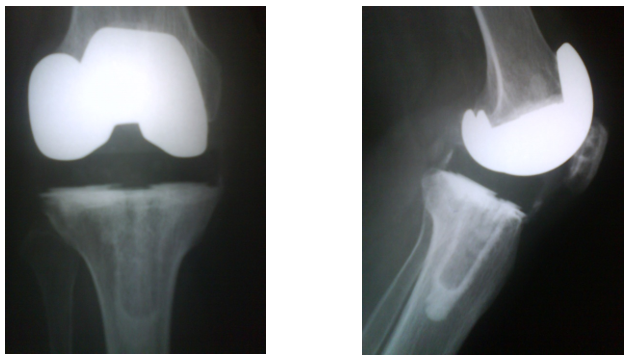
Figure 6: Plain radiograph of a patient showing no Osteolysis
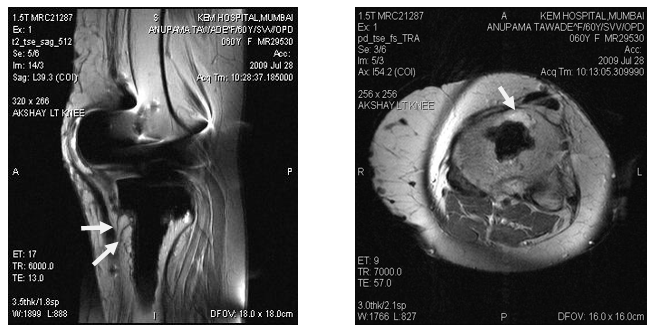
Figure 7: MRI showing Tibial Osteolysis
Osteolysis secondary to particulate debris is an increasingly recognized cause of periprosthetic bone loss and failure of knee arthroplasty. Plain radiographs are the most common method of surveillance for the presence and progression of osteolysis, yet the amount of osteolysis present are underestimated frequently by this radiographic modality. Better characterization of the extent and location of osteolysis preoperatively provides for improved planning with respect to the volume of bone graft and prosthetic options inventory at surgery and more informed clinical decision making about the need for reoperation.
MRI as a tool to detect osteolysis:
Vessely et al was the first to use MRI specifically for osteolysis. A study of 28 hip arthroplasties by [13] demonstrated good association between MRI and plain radiographs in determining the presence and extent of osteolysis.
Our study of 22 knees is specifically aimed at osteolysis detection in long term post-operative TKA patients in detecting the osteolysis.
Calculation of the size of osteolysis:
[24] had detected osteolytic lesions on radiographs and quantified by measuring 3 dimensions and thereby calculating the volume. They showed that MRI demonstrated secondary osteolytic lesions which were radiographically occult. (55%). The 11 patients selected by them were suspected of having osteolysis on plain radiographs. In our study our observation suggests that osteolysis was detected on MRI in 45% patients, out of these 25% of the lesions were radiographically occult. MRI thus showed that plain radiographs are far less sensitive in detecting early osteolysis. (50% less).
Plain radiographs being a 2-dimensional modality we after eliminating interobserver variability calculated only the two longest dimensions and thereby estimated the approximate area. MRI showed a 3-dimensional view of the lesion and therefore volume could be calculated. (Average area -260mm2, Average volume-5794mm3)
As shown by earlier studies, incidence of osteolysis was more in tibia than the femur. On plain radiographs there was 50% more incidence of osteolysis on tibial side. MRI showed 10% more as compared to femur. Also, other findings like synovial debris were seen.
A study by [25] demonstrated that the sensitivity of MRI for detection of osteolytic lesions in a cadaveric model (95%) was significantly better than that offered by conventional radiographic analysis (52%) or optimized CT (75%) and also demonstrated that sensitivity increased for all 3 imaging modalities as the lesion size increased but that lesion detection was independent of location only with MRI.
In our study, we had retrospectively reviewed 22 knees (asymptomatic and symptomatic) that had been operated more than 5 years before, specifically for osteolysis using plain radiographs and MRI. We had calculated area of the osteolytic lesion on plain radiograph and volume on MRI.
Our study was able to show:
MRI as a 3-dimensional modality to detect the size of the osteolytic lesions fairly accurately was superior to plain radiographs as a 2-dimensional modality. (Average area on plain radiograph-260mm2, Average volume on MRI-5794mm3)
MRI as an effective modality to pick up early lesions in asymptomatic knees which are not evident on plain radiograph.
MRI has an added advantage to detect other soft tissue pathology.
Limitations of our investigation include modest sample size. Radiography being a 2-dimensional modality only approximate area could be calculated. This also could not be compared with MRI as a 3-dimensional modality in which volume was estimated fairly accurately. Another aspect remains to be studied is the comparison of MRI with CT scan in detecting osteolysis. The findings of MRI could not be confirmed intraoperatively as no patient had undergone revision surgery.
Thus, we recommend that MRI can be used as a routine investigation in more than 5 to 10 years post-operative TKA patients to detect early lesions (plain radiograph negative, MRI positive) and do timely intervention.
The current study demonstrates the use of this technology to detect early osteolysis in patients who are otherwise asymptomatic and those who are symptomatic due to osteolysis as shown by plain radiograph, to demonstrate the accurate 3-dimensional quantification of the lesion. In conclusion, this study was able to demonstrate that MRI, with modification of pulse sequence parameters to reduce metallic susceptibility artefact and improve image quality, can be used for early detection of osteolysis.
The use of MRI in the assessment of patients with possible complications related to TKA is an evolving area, and additional refinement and clinical correlation will further elucidate the optimal applications of this technique.
Osteolysis is one of the major problems in TKA patients and an important aetiology for revision surgeries. MRI with metal artefact suppression can fairly accurately detect early lesions and measure them. MRI seems to be a superior modality in this respect as compared to plain radiographs.
Early detection and timely intervention in the form of treatment for the lesions thus will reduce the need for frequent revision TKA.
RANAWAT, CHITRANJAN S., WILLIAM F. FLYNN JR, Stephen Saddler, Kenneth K. Hansraj, and Michael J. Maynard. "Long-term results of the total condylar knee arthroplasty: a 15-year survivorship study." Clinical Orthopaedics and Related Research® 286 (1993): 94-102.
Hofmann, Aaron A., Scott M. Heithoff, and Marcelo Camargo. "Cementless total knee arthroplasty in patients 50 years or younger." Clinical Orthopaedics and Related Research (1976-2007) 404 (2002): 102-107.
Berry, Daniel J. "Recognizing and identifying osteolysis around total knee arthroplasty." Instructional Course Lectures 53 (2004): 261-264.
Wasielewski, Ray C., Nancy Parks, Ian Williams, Helene Surprenant, John P. Collier, and Gerard Engh. "Tibial insert undersurface as a contributing source of polyethylene wear debris." Clinical Orthopaedics and Related Research (1976-2007) 345 (1997): 53-59.
Nadaud, Matthew C., Thomas K. Fehring, and Keith Fehring. "Underestimation of osteolysis in posterior stabilized total knee arthroplasty." The Journal of arthroplasty 19, no. 1 (2004): 110-115.
Wright, T., and S. Goodman. "Implant Wear: The future of Joint Replacement." American Academy of Orthopaedic Surgeons, Rosemont, IL (1995).
Fehring, Thomas K., Susan Odum, William L. Griffin, J. Bohannon Mason, and Matthew Nadaud. "Early failures in total knee arthroplasty." Clinical Orthopaedics and Related Research (1976-2007) 392 (2001): 315-318.
Cadambi, Ajai, Gerard A. Engh, Kimberly A. Dwyer, and Tuyethoa N. Vinh. "Osteolysis of the distal femur after total knee arthroplasty." The Journal of arthroplasty 9, no. 6 (1994): 579-594.
HC, AMSTUTZ. "Mechanism and clinical significance of wear debris-induced osteolysis." Clin Orthop 276 (1992): 7-18.
Engh Jr, C. Anderson, Christi J. Sychterz, Anthony M. Young, David C. Pollock, Sean D. Toomey, and Charles A. Engh Sr. "Interobserver and intraobserver variability in radiographic assessment of osteolysis." The Journal of arthroplasty 17, no. 6 (2002): 752-759.
Gupta, Sanjay K., Alice Chu, Amar S. Ranawat, John Slamin, and Chitranjan S. Ranawat. "Osteolysis after total knee arthroplasty." The Journal of arthroplasty 22, no. 6 (2007): 787-799.
Peters Jr, PAUL C., G. A. Engh, K. A. Dwyer, and T. N. Vinh. "Osteolysis after total knee arthroplasty without cement." JBJS 74, no. 6 (1992): 864-876.
Potter, Hollis G., Bryan J. Nestor, Carolyn M. Sofka, Stephanie T. Ho, Lance E. Peters, and Eduardo A. Salvati. "Magnetic resonance imaging after total hip arthroplasty: evaluation of periprosthetic soft tissue." JBJS 86, no. 9 (2004): 1947-1954.
Lewis, P. L., C. H. Rorabeck, and R. B. Bourne. "Screw osteolysis after cementless total knee replacement." Clinical Orthopaedics and Related Research® 321 (1995): 173-177.
Robinson, Eric J., Brian D. Mulliken, Robert B. Bourne, Cecil H. Rorabeck, and Christine Alvarez. "Catastrophic Osteolysis in Total Knee Replacement." Clinical Orthopaedics and Related Research (1976-2007) 321 (1995): 98-105.
Jacobs JJ. Osteolysis: basic science. Clin Orthop Relat Res 2001;393.
Shanbhag, Arun S., Hallum O. Bailey, Deuk‐Soo Hwang, Charles W. Cha, Nicholas G. Eror, and Harry E. Rubash. "Quantitative analysis of ultrahigh molecular weight polyethylene (UHMWPE) wear debris associated with total knee replacements." Journal of Biomedical Materials Research: An Official Journal of The Society for Biomaterials, The Japanese Society for Biomaterials, and The Australian Society for Biomaterials and the Korean Society for Biomaterials 53, no. 1 (2000): 100-110.
Horikoshi, M. "Comparison of interface membranes obtained from failed cemented and cementless hip and knee prosthesis." Clin Orthop 309 (1994): 369-387.
Athanasou, N. A., J. Quinn, and C. J. Bulstrode. "Resorption of bone by inflammatory cells derived from the joint capsule of hip arthroplasties." The Journal of Bone & Joint Surgery British Volume 74, no. 1 (1992): 57-62.
Kovacik, Mark W., Ivan A. Gradisar Jr, John J. Haprian, and Thomas S. Alexander. "Osteolytic indicators found in total knee arthroplasty synovial fluid aspirates." Clinical Orthopaedics and Related Research (1976-2007) 379 (2000): 186-194.
Callaghan, John J., Matt W. Squire, Devon D. Goetz, Patrick M. Sullivan, and Richard C. Johnston. "Cemented rotating-platform total knee replacement: a nine to twelve-year follow-up study." JBJS 82, no. 5 (2000): 705.
Minkin, Cedric. "Bone acid phosphatase: tartrate-resistant acid phosphatase as a marker of osteoclast function." Calcified tissue international 34, no. 1 (1982): 285-290.
Vessely, Michael B., Matthew A. Frick, Daniel Oakes, Doris E. Wenger, and Daniel J. Berry. "Magnetic resonance imaging with metal suppression for evaluation of periprosthetic osteolysis after total knee arthroplasty." The Journal of arthroplasty 21, no. 6 (2006): 826-831.
The Journal of Arthroplasty Vol. 21 No. 6 2006
Walde, Tim A., Daniel E. Weiland, Serena B. Leung, Nobuto Kitamura, Christi J. Sychterz, C. Anderson Engh Jr, Alexandra M. Claus, Hollis G. Potter, and Charles A. Engh Sr. "Comparison of CT, MRI, and radiographs in assessing pelvic osteolysis: a cadaveric study." Clinical Orthopaedics and Related Research® 437 (2005): 138-144.
Lonner, Jess H., John M. Siliski, and Richard D. Scott. "Prodromes of failure in total knee arthroplasty." The Journal of arthroplasty 14, no. 4 (1999): 488-492.
Cooper, H. John, Amar S. Ranawat, Hollis G. Potter, Li Foong Foo, Shari T. Jawetz, and Chitranjan S. Ranawat. "Magnetic resonance imaging in the diagnosis and management of hip pain after total hip arthroplasty." The Journal of Arthroplasty 24, no. 5 (2009): 661-667.
Dl, Bartel. "The effect of conformity, thickness, and material on stresses in ultrahighmolecular weight components for total joint replacement." J Bone Joint Surg 68 (1986): 1041-1051.
Puloski, S. K. T., R. W. McCalden, S. J. MacDonald, C. H. Rorabeck, and R. B. Bourne. "Tibial post wear in posterior stabilized total knee arthroplasty: an unrecognized source of polyethylene debris." JBJS 83, no. 3 (2001): 390.
Fehring, Thomas K., Jeffrey A. Murphy, T. David Hayes, Donald W. Roberts, Donald L. Pomeroy, and William L. Griffin. "The Coventry Award Paper: Factors Influencing Wear and Osteolysis in Press-Fit Condylar Modular Total Knee Replacements." Clinical Orthopaedics and Related Research (1976-2007) 428 (2004): 40-50.
McEwen, H. M. J., P. I. Barnett, C. J. Bell, R. Farrar, D. D. Auger, M. H. Stone, and J. Fisher. "The influence of design, materials and kinematics on the in vitro wear of total knee replacements." Journal of biomechanics 38, no. 2 (2005): 357-365.
Muratoglu, Orhun K., Charles R. Bragdon, Daniel O. O'Connor, Murali Jasty, and William H. Harris. "A novel method of cross-linking ultra-high-molecular-weight polyethylene to improve wear, reduce oxidation, and retain mechanical properties: recipient of the 1999 HAP Paul Award." The Journal of arthroplasty 16, no. 2 (2001): 149-160.
Fisher, John, Hannah MJ McEwen, Joanne L. Tipper, Alison L. Galvin, Jo Ingram, Amir Kamali, Martin H. Stone, and Eileen Ingham. "Wear, debris, and biologic activity of cross-linked polyethylene in the knee: benefits and potential concerns." Clinical Orthopaedics and Related Research (1976-2007) 428 (2004): 114-119.
Ezzet, Race A., Rolando Garcia, and Robert L. Barrack. "Effect of component fixation method on osteolysis in total knee arthroplasty." Clinical Orthopaedics and Related Research® 321 (1995): 86-91.
Puri, Lalit, Richard L. Wixson, Steven H. Stern, Joe Kohli, Ronald W. Hendrix, and S. David Stulberg. "Use of helical computed tomography for the assessment of acetabular osteolysis after total hip arthroplasty." JBJS 84, no. 4 (2002): 609-614.