Shakuntala Chhabra1*, Naina Kumar2
1Senior consultant, Obstetrics Gynecology, Shri Vile Parle Kelvani Mandal’s Tapan Bhai Mukesh Bhai Patel Memorial Hospital, Medical College, and Research Centre, Kharde, Shirpur, Dhule, Maharashtra, India
2 Additional Professor, Obstetrics Gynecology, All India Institute of Medical Sciences, Hyderabad Metropolitan Region, Telangana, India
*Correspondence: Shakuntala Chhabra, Senior consultant, Obstetrics Gynecology Shri Vile Parle Kelvani Mandal’s Tapan Bhai Mukesh Bhai Patel Memorial Hospital, Medical College, and Research Centre, Kharde, Shirpur, Dhule, Maharashtra, India. Email:chhabra_s@rediffmail.com/drschhabra22@ gmail.com/shakuntala.chhabra@svkm.ac.in ORCID Number: https://orcid.org/0000-0003-1994-3474
Received: 08 Oct, 2025; Accepted: 25 Oct, 2025; Published: 05 Nov, 2025.
Citation: Shakuntala Chhabra and Naina Kumar. “Impact of Biomass Fuel Usage on Hypertensive Disorders in Pregnant Women: A Community-Based Study in a Rural, Remote, Hilly Region” J Gynecol Matern Health (2025): 117. DOI: 10.59462/3068-3696.3.1.117
Copyright: © 2025 Shakuntala Chhabra. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: Hypertensive disorders of pregnancy (HDsP) are common complications of pregnancy.
Objective: To know impact of biomass fuel use and effects of feasible actions to reduce impact on HDsP in pregnant women.
Methodology: Community-based study was conducted in 100 villages around village with health facility (study center) with normotensive women of early gestation. Villages were randomly divided into 50 study, 50 control villages. Study villages were further subdivided into 40, where advocacy about protection from biomass fuel effects was done, 10 where with advocacy, chimneys were also fixed on rooftops, in control villages neither advocacy was done nor chimneys were fixed. Information about occurrence of HDsP, their severity, pregnancy outcome was collected by research assistants by interviews of pregnant, post-birth women and looking at their maternity records through village visits on regular basis. However, blood pressure was recorded by research assistants in every visit. It was not case-control, but control, study villages. Results: There were 3,400 births in study, 2,818 in controls. In 40 study villages, 79.1% women used biomass fuel,20.9% did not. In 10 villages with advocacy and chimneys, 73.9% used biomass fuel, 26.1% did not. In 50 control villages, 81.2% used biomass fuel, 18.8% did not. Significant differences in HDsP were revealed between biomass users in advocacy villages (40), biomass-users of advocacy with chimneys villages (10), and biomass users in control villages (50). Incidence, number of severe cases of HDsP, eclampsia was lowest in 10 study villages.
Conclusion: Biomass fuel usage had significant impact on occurrence, severity of HDsP, actions made significant difference.
Keywords: Rural women, Biomass fuel, Hypertensive disorders of pregnancy, Indoor air pollution, Impact, Actions
Synopsis: Biomass fuel usage was significantly associated with occurrence, severity of HDsP, and actions made real impact in reduction.
Introduction
According to the World Health Organization (WHO), approximately 2.3 billion people worldwide still rely on solid fuels, such as wood, coal, charcoal, agricultural residues, and animal dung for household cooking [1]. A study from India revealed that about 64% of households used solid fuels, with a higher prevalence in rural (81%) compared to urban (26%) [2]. The biomass fuels release various harmful gases and pollutants, including particulate matter, carbon monoxide, nitrogen dioxide, and carcinogenic organic air pollutants [3,4]. The adverse effects of biomass smoke exposure are particularly severe for women, who typically do the cooking, and on babies who are always around [5]. Numerous studies from all over the world have revealed a strong relationship between the usage of biomass fuel at home and occurrence of hypertension in men and non-pregnant women, however, the association between biomass fuel usage and the occurrence of hypertension during pregnancy remains ambiguous [6,7]. Hypertensive disorders during pregnancy (HDsP) are one of the most common complications during pregnancy, affecting 10% of all pregnancies globally [8] and are associated with adverse maternal, and perinatal outcomes [9]. There is lack of reported studies investigating the relationship between the use of solid fuels for cooking, water heating, and heating for protection from cold, and the occurrence of HDsP. Additionally, evidence on the impact of any interventions, particularly rural community-based is limited. Some studies that tried to find the relationship between the type of cooking fuel and HDsP have revealed inconsistent results [10,11].
The present community-based interventional study was conducted to know the impact of biomass fuel use on occurrence of HDsP and also the impact of interventions in pregnant women who resided in the rural, forestry hilly region.
Material and methods
Study setting: The community-based study was carried out amongst tribal communities in 100 villages around the village with a health facility (study center), in a remote, forestry and hilly region.
Study Design: Community-based study.
Study period: Two years
Inclusion criteria: All women residing in 100 villages around the village with health facility (study center), diagnosed with pregnancy, beginning of second
trimester, having normal blood pressure, no anti hypertensive treatment or any known major illness, willing to be a part of the study and delivered during the study period were the study participants.
Exclusion criteria: Nonpregnant women, those with advanced pregnancy, post-partum and post-aborted women, those with any known major illness, including hypertension, and those not willing to be a part of the study were excluded, however, no one refused.
Sampling technique: Except for a few migrants, all women of study villages who gave birth in the villages during the study period and fulfilled inclusion criteria were included, so sample size calculation was not done.
Data collection
Following approval from the institute’s ethics committee and obtaining informed consent from participants, present prospective study was conducted across 100 villages over a period of two years. The study adhered to the CONSORT guidelines. A predesigned tool was used for collecting information by the trained field assistants. None of the participants was given the tool to fill out. Villages of the region were similar in context of huts and living conditions. All 100 villages of study were randomly divided into two groups, 50 study villages and 50 controls, using a lottery system. The study villages were further subdivided into two groups, group I consisted of 40 villages where advocacy for protection from the smoke of biomass fuel was done at regular intervals, and Group II consisted of 10 villages (randomly selected by a lottery system) where in addition to the advocacy for protection from smoke, chimneys were also installed on rooftops of huts lacking windows, for exit of biomass fuel smoke. In control 50 villages, neither advocacy for protection from biomass fuel smoke was done, nor were chimneys installed. Details of pregnant women, including age, education, occupation, economic status, parity, and outcome, were collected by research assistants by asking women and seeing records of their maternity care and perinatal outcome. While information about HDsP was collected from women’s maternity records, blood pressure was also measured by the research assistant. During the village visit, if blood pressure was found to be high (≥140/90 mmHg) on two occasions, four hours apart, a diagnosis of HDsP was made at the referral hospital, study center. Many investigations could not be done in many, so workup was not part of the study, a limitation of the community-based study in remote villages with scarce resources.
The maternal and perinatal outcomes in the study and control villages were analyzed and compared to know the impact of biomass fuel usage on pregnant women and the impact of low-cost interventions. Figure 1 depicts the CONSORT flow diagram of the methodology of the study.
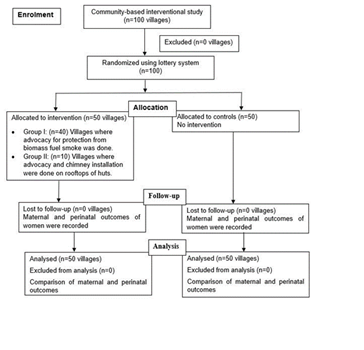
Figure 1: CONSORT flow diagram depicting the Methodology of the study
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) software, version 21.0. Categorical variables were summarized as frequencies and percentages, and comparisons between groups were conducted using the chi-square test. A p-value of <0.05 was considered statistically significant.
Results
The 50 study and 50 control villages, randomly allocated, had comparable baseline characteristics. On comparing study and control villages, it was revealed that a total of 2652 (78.0%) women reported the use of biomass fuel, and 748 (22.0%) did not in 50 study villages, and in 50 control villages, 2287 (81.2%) women reported use of biomass fuel and 531 (18.8%) did not.
There was a total of 3400 births in 50 study villages (40+10 villages). Of the 40 study villages where advocacy regarding protection from biomass fuel smoke was done at every visit, at least monthly, 2135(62.8%) women reported the use of biomass fuel for cooking, water heating, and heating of their homes. Of these 2135 women in study villages, the majority were of 20-29 years of age (57.1%), illiterate (40.6%), homemakers (48.9%), belonged to the low economic class (49.0%), and had 2-3 children (52.9%). Of 2135 women who were exposed to biomass fuel smoke, 1913 (89.6%) remained normotensive, and 222(10.4%) were diagnosed with HDsP. Of these 222 women with HDsP, 153 (68.9%) had moderate hypertension, 99(64.7%) at term and 54(35.3%) at preterm gestation, 54 (24.3%) had severe hypertension (mainly based on blood pressure), 38 (70.3%) at term and 16 (29.6%) at preterm gestation, and 15 (6.8%) had eclampsia, 11 (73.3%) at term and four (26.7%) at preterm gestation. In the 40 study villages with advocacy, a total of 565 pregnant women reported no use of biomass fuel, the majority were of 20-29 years of age (67.3%), middle or high school educated (48.5%), with semi skilled occupation (29.7%), belonged to middle upper economic class (27.8%), and had 2-3 children (53.3%). Of these 565 non-biomass fuel user women, 515 (91.2%) remained normotensive, and 50 (8.8%) developed HDsP, 33 (66.0%) developed moderate hypertension, 20 (60.6%) at term and 13 (39.4%) at preterm gestation, 11 (22.0%) developed severe hypertension, five (45.5%) at term and six (54.5%) at preterm gestation, and six (12.0%) developed eclampsia, three (50.0%) at term and three (50.0%) at preterm gestation. Table I depicts the comparison of HDsP among biomass fuel users and non-users in relation to various socio-demographic parameters in 40 study villages (Table 1).
Overall, in the 40 study villages, among a total of 2700 pregnant women, 2135 (79.1%) used biomass fuel, and 565 (20.9%) women did not use biomass fuel. Furthermore, it was observed that of the 2700 women, 222 (8.2%) women who developed HDsP were biomass fuel users compared to only 50 (1.9%) nonusers of biomass fuel (p=0.278).
| Variables | Total Biomass fuel users | Normotensive (%) | HDsP | Total Non-biomass fuel users (%) N=565 | Normotensive (%) | HDsP (%) | Chi-square | p-value |
| (%) N=2135 | (%) | |||||||
| AGE (Years) | ||||||||
| ≥15-≤19 | 719 (33.7) | 634(88.2) | 85(11.8) | 178(13.5) | 161(90.4) | 17(9.5) | 0.729 | 0.393 |
| ≥20-≤29 | 1220 (57.1) | 1101(90.2) | 119(9.8) | 380(67.3) | 347(91.3) | 33(8.7) | 0.385 | 0.353 |
| ≥30-≤39 | 196 (9.2) | 178(90.8) | 18(9.2) | 07(1.2) | 07(100.0) | 0(0.0) | 0.702 | 0.402 |
| EDUCATION | ||||||||
| Illiterate | 866(40.6) | 762(88.0) | 104(12.0) | 47(8.3) | 38(80.8) | 09(19.2) | 2.093 | 0.148 |
| Primary | 602(28.2) | 538(89.4) | 64(10.6) | 68(12.0) | 57(83.8) | 11(16.2) | 1.887 | 0.169 |
| Middle/High school | 567(26.6) | 519(91.5) | 48(8.5) | 274(48.5) | 249(90.9) | 25(9.11) | 0.1 | 0.751 |
| Graduate | 59(2.8) | 55(93.2) | 04(6.8) | 116(20.5) | 112(96.5) | 04(3.4) | 0.989 | 0.319 |
| Postgraduate | 41(1.9) | 39(95.1) | 02(4.9) | 60(10.6) | 59(98.3) | 01(1.7) | 11.123 | 0.001 |
| OCCUPATION | ||||||||
| Homemakers | 1043(48.9) | 937(89.8) | 106(10.2) | 129(22.8) | 117(90.7) | 12(9.3) | 0.094 | 0.759 |
| Unskilled | 791(37.0) | 705(89.1) | 86(10.9) | 129(22.8) | 116(89.9) | 13(10.1) | 94.525 | 0.001 |
| Semi-skilled | 217(10.2) | 195(89.8) | 22(10.1) | 168(29.7) | 152(90.5) | 16(9.5) | 0.04 | 0.843 |
| Skilled | 54(2.5) | 49(90.7) | 05(9.3) | 93(16.5) | 86(92.5) | 07(7.5) | 0.136 | 0.713 |
| Business | 30(1.4) | 27(90.0) | 03(10.0) | 46(8.1) | 44(95.6) | 02(4.3) | 0.931 | 0.334 |
| ECONOMIC STATUS | ||||||||
| Upper | 13(0.6) | 12(92.3) | 01(7.7) | 55(9.7) | 53(96.4) | 02(3.6) | 0.404 | 0.525 |
| Middle upper | 61(2.9) | 55(90.2) | 06(9.8) | 157(27.8) | 150(95.5) | 07(4.4) | 2.255 | 0.133 |
| Middle | 249(11.7) | 229(92.0) | 20(8.0) | 145(25.7) | 134(92.4) | 11(7.6) | 0.025 | 0.874 |
| Middle lower | 765(35.8) | 682(89.2) | 83(10.8) | 110(19.5) | 90(81.8) | 20(18.2) | 4.973 | 0.026 |
| Lower | 1047(49.0) | 935(89.8) | 112(10.2) | 98(17.3) | 88(89.8) | 10(10.2) | 0.023 | 0.879 |
| PARITY | ||||||||
| P1 | 845(39.6) | 767(90.8) | 78(9.2) | 260(46.0) | 235(90.4) | 25(9.6) | 0.035 | 0.852 |
| P2-P3 | 1129(52.9) | 1014(89.8) | 115(10.2) | 301(53.3) | 276(91.7) | 25(8.3) | 0.951 | 0.329 |
| >P4-P5 | 161(7.5) | 132(82.0) | 29(18.0) | 04(0.7) | 04(100.0) | 00(0.0) | 0.869 | 0.351 |
|
P: Parity; HDsP: Hypertensive disorders of pregnancy The chi-square test was applied to examine relationships between categorical variables. A p-value <0.05 was considered statistically significant |
||||||||
Table 1: Comparison of Hypertensive Disorders during Pregnancy Among Biomass fuel users and non-users in relation to vari ous Socio-demographic parameters in 40 study villages
In the 10 study villages where chimneys were also fixed on the rooftops of huts with poor ventilation, there were a total of 700 pregnant women. Of these 700 women, 517 (73.9%) reported the use of biomass fuel in their houses, and 183 (26.1%) did not use biomass fuel. Of the 517 women exposed to biomass fuel smoke, 483 (93.4%) remained normotensive and 34 (6.6%) developed HDsP. Of these 34 hypertensive women, 29 (85.3%) developed moderate hypertension, 14 (48.3%) at term and 25 (51.7%) at preterm gestation, five (14.7%) developed severe hypertension, two (40.0%) at term and three (60.0%) at preterm gestation, and none of the women developed eclampsia in these villages.
Of 183 women in 10 study villages who did not use biomass fuel, 173 (94.5%) remained normotensive, and 10 (5.5%) developed HDsP. Of these hypertensive women, 08 (80.0%) developed moderate hypertension, only two (20.0%) had severe hypertension, and none eclampsia. Table II depicts the comparison of HDsP among biomass fuel users and non-users in relation to various socio-demographic parameters in 10 study villages (Table 2).
| Variables | Total Biomass fuel users | Normotensive | HDsP | Total Biomass fuel Non-users (%) N=183 | Normotensive | HDsP | Chi-square | p-value |
| (%) N=517 | (%) | (%) | (%) | (%) | ||||
| AGE (Years) | ||||||||
| ≥15-≤19 | 189(36.6) | 175(92.5) | 14(7.6) | 98(53.6) | 92(93.8) | 06(6.2) | 0.164 | 0.686 |
| ≥20-≤29 | 273(52.8) | 255(93.4) | 18(6.6) | 83(45.4) | 79(95.2) | 04(4.8) | 0.345 | 0.557 |
| ≥30-≤39 | 55(10.6) | 53(96.4) | 02(3.6) | 02(1.1) | 02(100.0 | 00(0.0) | 0.074 | 0.786 |
| EDUCATION | ||||||||
| Illiterate | 181(35.0) | 167(92.4) | 14(7.7) | 52(28.4) | 48(92.3) | 04(7.9) | 0 | 0.992 |
| Primary | 248(48.0) | 232(93.5) | 16(6.5) | 39(21.3) | 37(94.8) | 02(5.1) | 19.351 | 0.001 |
| Middle / High school | 69(13.3) | 65(93.8) | 04(5.8) | 70(38.3) | 67(95.7) | 03(4.3) | 0.165 | 0.685 |
| Graduate | 11(2.1) | 11(95.8) | 00(0.0) | 13(7.1) | 12(92.3) | 01(7.7) | 0.101 | 0.751 |
| Post Graduate | 08(1.5) | 08(95.0) | 00(0.0) | 09(4.9) | 09(100.0) | 00(0.0) | - | - |
| OCCUPATION | ||||||||
| Homemakers | 236(45.6) | 220(93.4) | 16(6.8) | 27(14.8) | 25(92.6) | 02(7.4) | 12.733 | 0.002 |
| Unskilled | 210(40.6) | 197(91.6) | 13(6.2) | 37(20.2) | 34(91.9) | 03(8.1) | 13.427 | 0.002 |
| Semi-skilled | 42(8.1) | 39(92.4) | 03(7.1) | 54(29.5) | 51(94.4) | 03(5.5) | 0.1001 | 0.751 |
| Skilled | 19(3.7) | 18(97.8) | 01(5.3) | 48(26.2) | 46(95.8) | 02(4.2) | 4.063 | 0.044 |
| Business | 10(1.9) | 10(100.0) | 00(0.0) | 17(9.3) | 17(100.0) | 00(0.0) | - | - |
| ECONOMIC STATUS | ||||||||
| Upper | 07(1.4) | 07(100.0) | 00(0.0) | 10(5.5) | 10(100.0) | 00(0.0) | - | - |
| Middle Upper | 12(2.3) | 11(91.7) | 01(8.3) | 22(12.0) | 22(100.0) | 00(0.0) | 1.833 | 0.178 |
| Middle | 58(11.2) | 54(93.1) | 04(6.9) | 61(33.3) | 59(96.7) | 02(3.3) | 0.806 | 0.369 |
| Middle Lower | 156(30.2) | 151(96.8) | 05(3.2) | 68(37.2) | 63(92.6) | 05(7.4) | 1.902 | 0.168 |
| Lower | 284(54.9) | 260(91.5) | 24(8.5) | 22(12.0) | 19(86.4) | 03(13.6) | 0.68 | 0.409 |
| PARITY | ||||||||
| P1 | 166(32.1) | 153(92.2) | 13(7.6) | 73(39.9) | 69(94.5) | 04(5.5) | 0.423 | 0.516 |
| P2-P3 | 337(65.2) | 316(93.8) | 21(6.3) | 110(60.1) | 104(94.5) | 06(5.5) | 0.088 | 0.767 |
| >P4-P5 | 14(2.7) | 14(100.0) | 00(0.0) | 00(0.0) | 00(0.0) | 00(0.0) | - | - |
| P: Parity; HDsP: Hypertensive disorders of pregnancy The chi-square test was applied to examine relationships between categorical variables. A p-value <0.05 was considered statistically significant |
||||||||
Table 2: Comparison of Hypertensive Disorders during Pregnancy Among Biomass fuel users and non-users in relation to vari ous Socio-demographic parameters in 10 study villages
In 10 study villages, of 700 women, 517 (73.9%) were biomass fuel users, and 183 (26.1%) were non-users. Of these 700 women, 34 (4.9%) women who developed HDsP were biomass fuel users compared to only 10 (1.4%) women who were non-biomass fuel users (p=0.595).
In 50 control villages where no action was taken, there were a total of 2818 births. Of these 2818 women, 2287(81.2%) reported biomass fuel usage, and 531 (18.8%) did not use biomass fuel. Of the 2287 users of biomass fuel, the majority were between 20-29 years (53.3%), illiterate (41.3%), and homemakers (51.1%), belonged to the low economic class (49.3%), and had 2-3 children (55.4%). Of these 2287 women exposed to biomass fuel smoke, 1964 (85.9%) remained normotensive and 323 (14.1%) developed HDsP. Of the hypertensive women, 221 (67.5%) developed moderate HDsP, 107 (48.4%) at term and 114 (51.6%) at preterm gestation, 72 (22.3%) developed severe HDsP, 33 (45.8%) at term and 39 (54.2%) at preterm gestation, and 30 (9.3%) developed eclampsia, 50.0% each at term and preterm gestation. Of 531 biomass fuel non-user women, 460 (86.6%) remained normotensive and 71 (13.4%) developed HDsP during pregnancy. Of these hypertensive women, 54 (76.1%) developed moderate hypertension, 30 (55.6%) at term and 24 (44.4%) at preterm gestation, 10 (14.1%) developed severe hypertension, 50.0% each at term and preterm gestation, and seven (9.9%) had eclampsia, four at term and three at preterm gestation. Table III depicts the comparison of HDsP among biomass fuel users and non-users in relation to various socio-demographic parameters in 50 control villages (Table 3). Overall, in 50 control villages, a total of 2818 births occurred, and it was revealed that 81.2% used biomass fuel and 18.8% women were biomass fuel nonusers. It was revealed that of 2818 women, 71.3% of women who had HDsP were biomass fuel users compared to only 28.7% who were biomass fuel nonusers (p=0.653).
| Variables | Total Biomass fuel | Normo- | HDsP (%) | Total Biomass fuel | Normo- | HDsP (%) | Chisquare | p-value |
| users (%) | tensive | Non-users | tensive | |||||
| N=2287 | (%) | (%) N=531 | (%) | |||||
| AGE (Years) | ||||||||
| ≥15-≤19 | 921(40.3) | 778(84.4) | 143(15.6) | 172(32.4) | 144(83.7) | 28(16.2) | 0.0621 | 0.803 |
| ≥20-≤29 | 1220(53.5) | 1055(86.5) | 165(13.5) | 354(66.7) | 311(87.8) | 43(12.1) | 0.4538 | 0.501 |
| ≥30-≤39 | 146(6.4) | 131(89.7) | 15(10.3) | 05(0.9) | 05(100.0) | 00(0.0) | 0.5666 | 0.452 |
| EDUCATION | ||||||||
| Illiterate | 944(41.3) | 771(81.7) | 173(18.3) | 62(11.7) | 41(66.1) | 21(33.9) | 0.4126 | 0.521 |
| Primary | 699(30.6) | 642(91.8) | 57(8.2) | 71(13.4) | 57(83.1) | 14(19.7) | 10.2832 | 0.001 |
| Middle | 533(23.3) | 443(83.1) | 90(16.9) | 248(46.7) | 223(89.9) | 25(10.1) | 6.2337 | 0.013 |
| / High school | ||||||||
| Graduate | 68(3.0) | 66(97.1) | 02(2.9) | 105(19.8) | 97(92.4) | 08(7.6) | 1.6487 | 0.199 |
| Post Graduate | 43(1.9) | 42(97.7) | 01(2.3) | 45(8.5) | 42(93.3) | 03(6.6) | 0.4647 | 0.495 |
| OCCUPATION | ||||||||
| Homemakers | 1169(51.1) | 991(84.8) | 178(15.2) | 128(24.1) | 110(85.9) | 18(14.0) | 0.1218 | 0.727 |
| Unskilled | 846(37.0) | 736(87.0) | 110(13.0) | 137(25.8) | 111(81.0) | 26(19.0) | 3.5283 | 0.06 |
| Semiskilled | 168(7.3) | 146(86.9) | 22(13.1) | 153(28.8) | 133(86.9) | 20(13.1) | 0 | 0.995 |
| Skilled | 66(2.9) | 58(87.9) | 08(12.1) | 83(15.6) | 78(93.9) | 05(6.0) | 1.7047 | 0.172 |
| Business | 38(1.7) | 33(86.8) | 05(13.1) | 30(5.6) | 28(93.3) | 02(6.6) | 0.7537 | 0.385 |
| ECONOMIC STATUS | ||||||||
| Upper | 14(0.6) | 13(92.9) | 01(7.1) | 42(7.9) | 41(97.6) | 01(2.4) | 0.679 | 0.41 |
| Middle Upper | 61(2.7) | 57(93.4) | 04(6.6) | 131(24.7) | 119(90.8) | 12(9.2) | 0.3672 | 0.545 |
| Middle | 242(10.6) | 218(90.1) | 24(9.9) | 137(25.8) | 117(85.4) | 20(14.6) | 1.8631 | 0.172 |
| Middle Lower | 843(36.9) | 726(86.1) | 117(13.9) | 146(27.5) | 121(82.9) | 25(17.1) | 1.0642 | 0.303 |
| Lower | 1127(49.3) | 950(84.3) | 177(15.7) | 75(14.1) | 62(82.7) | 13(17.3) | 0.1399 | 0.708 |
| PARITY | ||||||||
| P1 | 905(39.6) | 754(83.3) | 151(16.7) | 240(45.2) | 208(86.7) | 32(13.3) | 1.5856 | 0.208 |
| P2-P3 | 1266(55.4) | 1100(86.9) | 166(13.1) | 289(54.4) | 250(86.5) | 39(13.5) | 0.0301 | 0.862 |
| >P4-P5 | 116(5.1) | 110(94.8) | 06(5.2) | 02(0.4) | 02(100.0) | 00(0.0) | 0.1081 | 0.742 |
| P: Parity; HDsP: Hypertensive disorders of pregnancy | ||||||||
| The chi-square test was applied to examine relationships between categorical variables. A p-value <0.05 was | ||||||||
| considered statistically significant | ||||||||
Table 3: Comparison of Hypertensive Disorders during Pregnancy Among Biomass fuel users and non-users in relation to vari ous Socio-demographic parameters in 50 Control villages
The distribution of cases of HDsP across three groups of villages: 50 control villages, 40 villages with advocacy only, and 10 villages with advocacy and also chimney installation ,revealed that , while overall numbers of HDsP cases were significantly less in 40villages with only advocacy, much more impact was revealed in 10 villages where Chimneys were also fixed, however numbers with severity observed among biomass fuel users across the three groups were not statistically significantly different as numbers were small ,specially in 10 villages amongst biomass fuel users (p = 0.170) and the same thing was found in among biomass fuel non-users across the village categories (p = 0.594).
The present article is about the study of the effects of biomass fuel use on HDsP during pregnancy and the impact of low-cost interventions. Another study was conducted about the effects of biomass fuel in the context of babies, so a detailed analysis of perinatal outcome is not part of the present article, however, similar to the pattern observed with HDsP, there were notable differences in perinatal losses between biomass fuel users and non-users among those with HDsP. In the 40 advocacy villages, perinatal losses occurred in 10.8% of biomass users with HDsP compared to 8.7% of non-users. In the 10 villages with both advocacy and chimneys, the rates were 8.7% for users and 6.6% for non-users. In the 50 control villages, the disparity was more pronounced, with perinatal losses in 24.4% of users and 20.4% of non-users with HDsP.
Moreover, among women using biomass fuel, 256 cases of HDsP were reported in the 50 intervention villages, compared to 323 cases in the 50 control villages (p = 0.001). Among non-users of biomass fuel, 60 women in the study villages developed HDsP, compared to 71 in the control villages (p = 0.002). However, difference in the numbers with severity of HDsP observed between study and control villages among both biomass fuel users (p = 0.301) and non users (p = 0.514) was not statistically significant, probably because numbers in 10 villages were less.
A significant difference in the incidence of HDsP was observed between study villages that used biomass fuel and received only advocacy, and those that received advocacy and chimneys were installed (8.2% vs. 4.9%, respectively; p = 0.008). Similarly, when compared with the incidence of HDsP in pregnant women, a significant difference was found between 40 biomass-user study villages and 50 biomass-user control villages and a statistically significant difference was observed between 50 biomass fuel-users in control villages and 10 biomass-users in the study villages, where advocacy was done and chimneys were also installed .Table IV depicts the comparison in the occurrence of HDsP among pregnant women in 50 control villages, 40 study villages with advocacy alone, and 10 study villages with advocacy and chimney installation (Table 4).
| Blood Pressure | Villages | p-value | ||||
| Biomass fuel users in 50 control villages | Biomass fuel users in 40 study villages | Biomass fuel users in 10 study villages | Biomass fuel users in 50 control villages vs 40 study villages | Biomass fuel users in 50 control villages vs 10 study villages | Biomass fuel users in 40 study villages vs 10 study villages | |
| Normotensives | 1964 | 1913 | 483 | 0.001 | 0.001 | 0.008 |
| HDsP | 323 | 222 | 34 | |||
| Biomass fuel non-users in 50 control villages | Biomass fuel non-users in 40 study villages | Biomass fuel non-users in 10 study villages | Biomass fuel non-users in 50 control villages vs 40 study villages | Biomass fuel non-users in 50 control villages vs 10 study villages | Biomass fuel non-users in 40 study villages vs 10 study villages | |
| Normotensives | 460 | 515 | 173 | 0.017 | 0.004 | 0.143 |
| HDsP | 71 | 50 | 10 | |||
| The chi-square test was applied to examine relationships between categorical variables. A p-value <0.05 was considered statistically significant | ||||||
Table 4: Comparison of HDsP Incidence Among Pregnant Women in Control Villages, Advocacy-Only Villages, and Villages with Both Advocacy and Chimney Installation
Biomass fuel was commonly used in villages as a primary source for cooking and other household activities. More biomass fuel user women developed HDsP, more had severe disorder and adverse perinatal outcomes. Low-cost interventions, such as advocacy for the protection from the harmful effects of biomass fuel and the installation of chimneys on rooftops significantly reduced the incidence and severity of HDsP in pregnant women. Advocacy and chimneys installation not only affected the occurrence, numbers with severity but perinatal loss in HDsP, where higher perinatal loss is known.
Discussion
Main Findings:
The present community-based study was conducted in 100 villages, randomly divided with 50 villages as controls and 50 study villages, with some limitations, as the number of women in study and control villages were not the same. It was not case control cases but action taken and no action villages, as in villages, women meet at wells or river-banks and share information. A total of 78.0% of women reported the use of biomass fuel, and 22.0% did not use it in 50study villages and in 50 control villages, 81.2% of women reported use of biomass fuel, and 18.8% did not use it. In the study villages, 9.3% of women developed HDsP, 7.5% amongst biomass users, and 1.8% non-users. In control villages, a total of 14.0% of women developed HDsP, 11.5% biomass users, and 2.5% non-users. Furthermore, when compared with the incidence of HDsP, a significant difference was observed between 40 study villages amongst biomass fuel users and biomass fuel -users in50 control villages (p=0.001). A statistically significant difference was revealed in the incidence of HDsP between biomass fuel users in 50 control villages and 10 biomass-users in intervention villages where advocacy was done and chimneys were also installed (p=0.001). The incidence of HDsP and adverse perinatal outcomes were significantly different in 50 intervention villages compared to 50 control villages.
Interpretation:
The findings of the present study align with some other studies that have consistently demonstrated an association between household air pollution from the use of solid fuels and adverse pregnancy outcomes, particularly hypertensive disorders of pregnancy (HDP). A hospital-based study in China revealed that pregnant women using coal and other biomass fuel for cooking and heating had a higher risk for the development of pregnancy-induced hypertension (PIH) and preeclampsia compared to pregnant women using gas as cooking fuel [12]. Another recent community-based study from Tamil Nadu, India revealed that systolic blood pressure (SBP) and diastolic blood pressure (DBP) were higher in pregnant women exposed to higher levels of household air pollution due to the burning of solid fuels. A significant positive association was observed between exposure to carbon monoxide (CO) and DBP among pregnant women [13]. A community based randomized controlled study to assess the impact of liquefied petroleum gas stove and fuel intervention on household air pollution exposure and health in Guatemala, India, Peru, and Rwanda households that relied mainly on solid cooking fuels, revealed a moderate increase in SBP and DBP, in both the groups, but the increase was greater in the intervention group. It was observed that though the higher exposures to household air pollution were associated with a moderate increase in SBP and DBP, none of these associations were statistically significant. Hence, it was concluded that intervention with gas stoves in households using biomass fuels did not markedly affect gestational blood pressure in pregnant women [14]. Another study from India revealed that women using biomass and solid fuels for cooking and heating at homes had two times higher risk of developing preeclampsia/eclampsia compared to those living in households using cleaner fuels [10]. Contrary to the present community-based study, a hospital-based study conducted by other researchers in Indian villages revealed that women using wood as fuel lowered mean arterial pressure and diastolic blood pressure at delivery compared to gas users. Furthermore, it was found that was 14.6% women cooking with wood had hypertension compared to 19.6% for those cooking with gas [11]. Another hospital-based study conducted in Ghana to assess the impact of household fuel use on adverse pregnancy outcomes, revealed that using biomass fuels for cooking and heating was associated with an increased risk of perinatal mortality. However, the study observed no significant correlation between biomass fuel usage and the development of HDsP [15].
Limitations and future possibilities:
Present study was conducted in a low-resource rural setting, which may limit the generalizability of the findings to populations with different environmental, socio-economic, and health care access conditions, however smoke exposure in various forms is around the world which can also impact, and needs-based interventions can sure help. So, the results are important for the globe. Strict control measures for use are often not feasible in many settings. So, there is place of interventions. In the present study because of lack of finances, numbers of villages with chimneys could not be equalized, which did affect statistical differences, however for advocacy villages were equalized. Further the study did not include many diagnostics to fully capture the effects, that may be there because of the complexity of HDsP, a multi-organ condition.
Strengths:
Literature about exposure to biomass fuel and the development of HDsP especially community based prospective studies is scarce, but is very much needed as HDsP remain a leading cause of maternal and perinatal morbidity and mortality worldwide.
Community-based studies, especially in rural women, are very scarce. There are hardly any studies similar to the present and more studies are needed to know the effects and impact of possible interventions on HDsP as smoke with different contents is likely to come from various sources around the world. Smoke exposure of various forms can affect the health of everyone, more so pregnant women, and interventions are needed to reduce the impact. Future research should examine the effects of biomass fuel smoke and other sources of air pollution on pregnant women with more in-depth information to better understand the global burden of air pollution on maternal health and possibilities of modes of elimination.
Conclusion
The present study highlights a strong association between biomass fuel usage and HDsP, with significant differences in incidence, severity, and perinatal outcome in these cases across intervention and control villages. Compared to control villages, fewer women in intervention villages, where only advocacy was done, had HDsP and lesser severe cases also. The most significant impact was observed in the 10 villages where advocacy was done as well as chimneys were installed, leading to a further decline in the incidence and severity of HDsP and perinatal deaths. These findings underscore the need for targeted interventions, such as public health education and improved ventilation strategies, to mitigate the harmful effects of biomass fuel combustion on pregnant women and their newborns.
Disclosures
Author contributions
CS: Conceptualization, Planning, Literature search, Data collection, Formal analysis, Data
Interpretation, writing original draft, writing review and editing, final review, and approval of the manuscript.
KN: Literature search, Formal analysis, writing and editing, final review, and approval of the manuscript.
Conflict of Interests: The authors have no conflict of interest to declare.
Funding: Authors are grateful to the Indian Council of Medical Research, New Delhi India for funding the study, though funding was only for research in villages and intervention used.
References