Enyew Belay Getahun1*, Dr. Eshetu Tadele2, Dr Sisay T Mariam2, Dr Samson Gudu2, Tadelech Kelilie1
1Department Research and Training, Tirunesh Beijing Hospital, Addis Ababa, Ethiopia
2Departments of Obstetrics and Gynecology, Tirunesh Beijing Hospital, Addis Ababa, Ethiopia
*Correspondence: Enyew Belay Getahun, Department of Research and Training, Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, Email: enyewadress@gmail.com
Received: 21 Nov, 2025; Accepted: 05 Dec, 2025; Published: 16 Dec, 2025.
Citation: Getahun EB, Eshetu T, and Sisay TM et al. “Magnitude and Determinants of Shifting from Private to Public Health Facilities Among Pregnant Mothers with Previous Caesarean Scars Attending Public Hospitals, Addis Ababa, Ethiopia, 2025: A Cross-Sectional Study.” J Gynecol Matern Health (2025): 122. DOI: 10.59462/3068-3696.3.2.122
Copyright: © 2025 Enyew Belay Getahun. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Maternal healthcare in low- and middle-income countries, particularly in urban settings such as Addis Ababa, often relies on out-of pocket payments, leading patients to switch between the private and public health sectors. This study aims to assess burden of transition from Private to Public healthcare among Pregnant Women with Previous Cesarean Scars in Addis Ababa, Ethiopia (2025)
Methods: An institution-based cross-sectional study design was used to assess the magnitude and determinants of shifting from private to public health facilities among pregnant mothers with previous caesarean scars. The study was conducted from May 1, 2025, to June 15, 2025. A total of 422 women were taken. After taking four hospitals under Addis Ababa, administrative health bureau, Proportional allocation was done, and then each participant was selected systematically. Data was collected by structured questionnaire. The analysis was done by SPSS version 26 and in multivariable analysis those variables whose p-value was considered as statistically significant at p less than 0.05
Result: The study found that the magnitude of shifting from a private to a public health facility was 23.7% with a 95% CI: 19.4% to 27.8%). The multivariable analysis revealed that the Shifting behavior was significantly predicted by four key factors: Low family income (≤10,000 Br) was the strongest predictor, increasing the odds of shifting by nearly five times (AOR≈5); Higher educational attainment (above secondary) also showed a significant increase in the odds of shifting (over five times); Larger family size (≥3 members) was associated with approximately four times higher odds; and Advanced maternal age (≥35 years) significantly increased the likelihood of shifting (AOR=3.20).
Conclusion: Shifting of pregnant women with prior Cesarean Sections (CS) from private to public facilities in Addis Ababa is driven by financial struggles, particularly low income and large family size. However, older, educated women are also opting for public services due to their zero-cost nature, indicating growing trust in public health quality. This shift may overwhelm public hospitals, risking care quality. Private health facilities should consider financial subsidies for low-income families seeking private care, while public hospitals need to improve capacity and service segmentation. Additionally, private facilities should adopt competitive pricing and highlight non-financial benefits to attract the evolving patient demographics.
Keywords: Shifting, Public Health Facilities, Pregnant Mothers, Previous Caesarean Scars.
Introduction
Shifting from private to public health facilities among pregnant mothers with previous Caesarean scars is an increasing public health concern, particularly in low- and middle-income countries (LMICs) where healthcare systems are often strained. Globally, the rising rate of Caes arean sections (CS) has led to an increase in pregnancies with previous Caesarean scars, which are associated with higher risks of maternal and neonatal complications [1]. In such cases, the choice of healthcare facility for deliv ery is critical, as it can significantly influence maternal and fetal outcomes. While private health facilities often provide more personalized care, public health facilities are typ ically better equipped to handle high-risk deliveries due to their access to specialized staff, emergency services, and advanced medical equipment [2].
In sub-Saharan Africa, where maternal mortality rates remain disproportionately high, the shifting of pregnant women from private to public health facilities has been ob served as a response to the limitations of private health care providers in managing high-risk pregnancies [3]. Ethi opia, one of the countries in the region with a high maternal mortality ratio (MMR), faces significant challenges in pro viding equitable and quality maternal healthcare services. Despite efforts to improve healthcare access, disparities between private and public health facilities persist, particu larly in urban centres like Addis Ababa [4].
Addis Ababa has a mix of private and public health facili ties, yet the public sector remains the primary provider of maternal health services, especially for high-risk pregnan cies. Pregnant mothers with previous Caesarean scars often face complex clinical decisions regarding their de livery options. While some initially seek care in private facilities due to perceived better service quality, many eventually shifting to public hospitals as their pregnancy progresses, particularly when complications arise [5]. This shifting pattern raises important questions about the mag nitude and determinants of such transitions, as well as their implications for maternal health outcomes.
Understanding the factors driving this shifting is crucial for policymakers and healthcare providers to address gaps in service delivery and ensure that all pregnant women, re gardless of their risk profile, receive appropriate care. Pre vious studies have highlighted factors such as cost, perceived quality of care, availability of specialized services, and trust in healthcare providers as key determinants of facility choice among pregnant women [6]. However, there is limited evidence specifically focusing on pregnant mothers with previous Caesarean scars in Ethiopia, particularly in urban settings like Addis Ababa.
This study aims to fill this gap by examining the magnitude and determinants of shifting from private to public health facilities among pregnant mothers with previous Caesar ean scars attending public hospitals in Addis Ababa, Ethi opia, in 2025. By exploring the reasons behind this shifting and its impact on maternal health outcomes, the findings of this study will contribute to the development of targeted interventions to improve maternal healthcare services and reduce the burden of maternal morbidity and mortality in Ethiopia.
In Ethiopia, particularly in Addis Ababa, the choice of health facility for delivery among pregnant mothers with previous Caesarean scars is a critical public health concern [7]. These mothers are at a higher risk of complications such as uterine rupture, hemorrhage, and other obstetric emergencies, making the quality and type of health facility they choose for delivery a matter of life and death [8]. While private health facilities are often perceived to offer more personalized care and shorter waiting times, public health facilities are generally better equipped to handle high-risk deliveries due to their access to specialized staff, emergency obstetric care, and lower costs for patients [3].
However, there is an increasing trend of pregnant mothers with previous Caesarean scars migrating from private to public health facilities for delivery. This shift raises several questions: What is the magnitude of this shifting? What are the key determinants driving this decision? Are private facilities inadequately equipped to handle high-risk preg nancies, or are there other factors such as cost, perceived quality of care, or referral systems influencing this shifting?
Understanding the magnitude and determinants of this shifting is crucial for several reasons. First, it can inform policymakers and healthcare providers about the gaps in service delivery between private and public health facili ties. Second, it can help identify the specific needs of preg nant mothers with previous Caesarean scars, ensuring that they receive appropriate care regardless of the type of facility they choose. Third, it can guide the development of targeted interventions to improve the quality of care in both private and public health facilities, ultimately reducing maternal and neonatal morbidity and mortality.
Despite the importance of this issue, there is a lack of comprehensive data on the magnitude and determinants of shifting from private to public health facilities among pregnant mothers with previous Caesarean scars in Addis Ababa. This study aims to fill this gap by providing evidence-based insights that can inform policy and prac tice, ultimately contributing to improve maternal and child health outcomes in Ethiopia.
The study focuses on the shifting of pregnant mothers with previous Caesarean scars from private to public health fa cilities in Addis Ababa, Ethiopia, 2025. This shifting is a significant factor in improving maternal health outcomes, addressing healthcare inequities, and strengthening health systems. The research will identify gaps in care and improve the quality of maternal health services for these women.
It will also highlight disparities in healthcare ac cess and utilization, which are critical for achieving equit able healthcare delivery.
The study will also provide evidence to strengthen both private and public health facilities by identifying the de terminants of shifting. This can guide public hospitals in preparing for increased patient loads and improving ser vice delivery to meet the needs of high-risk pregnancies. Policymakers and healthcare planners will generate evi dence-based recommendations to address the factors driving shifting, such as regulating private healthcare pro viders, improving referral systems, or subsidizing care for high-risk pregnancies.
The study will also contribute to global knowledge by con tributing to the global body of knowledge on patient shifting and healthcare-seeking behaviour among high-risk popu lations. It will empower women and communities by pro viding better information and support for making informed choices about their care and raising awareness about the importance of skilled care for high-risk pregnancies.
In Ethiopia, the study will provide context-specific data to address challenges in urban areas like Addis Ababa where private and public health facilities coexist. By fo cusing on this high-risk group, the study will contribute to strengthening health systems, reducing maternal mortality, and ensuring equitable access to quality healthcare for all women.
Methods and Materials
Study Area
The study was conducted in Addis Ababa’s public hospitals. The city has a population density of 5,535.8 inhabit ants per square kilometre and occupies an estimated area of 174.4 square kilometers. There are also 11 sub-city health offices, which are directly accountable to their re spective sub-city administration. There are also 52 hospi tals in the metropolis of which 6 are owned by Addis Ababa regional health office AARHB, Five by federal government, 3 by NGO’s, 3 by Defence force and police and 35 by the private owners. There are 116 health centres owned by the city administration, and 3 by NGOs at present. There are also more than 760 private clinics at different levels (22). According to estimates from Ethiopia’s Central Statistical Agency, the Addis Ababa Region’s total population is es timated to be 5.55 million in 2017. Females in the repro ductive age group account for 35.5 percent of the overall population [9].
Study design
• An institutional based cross-sectional study design was used to assess the magnitude and determinants of shifting from private to public health facilities among pregnant mothers with previous caesarean scars from May1, 2025 to June 15, 2025.
Study Period
• The study was conducted from May 1, 2025 to June 15, 2025.
Population
Source Population
• All Pregnant mothers with previous caesarean scars attending public hospitals in Addis Ababa, Ethiopia.
Study populations
• All selected pregnant mothers with previous caesar ean scars attending selected public hospitals, Addis Ababa, Ethiopia, 2025
Inclusion and Exclusion Criteria
Inclusion Criteria
• Pregnant mothers with a history of at least one caes arean section and Mothers attending public hospitals for antenatal care or delivery in public hospitals, Addis Ababa, Ethiopia, 2025 during data collection period.
Exclusion Criteria
• Those participants who was severely ill was excluded from the study
Sample Size and Sampling Procedure
The Sample size was determined using single population proportion formula considering the following assumption: 95% confidence level (z α/2), 5% margin of error (d). Since there is no study found on expected proportion (p) of shifting from private to public health facilities among pregnant mothers with previous caesarean scars attending public hospitals. Therefor it was considered as 50% and sam pling was determined by single population proportion for mula as the following.
Where, P= 50 %
Z=level of confidence at 95% certainty (1.96) d= 5% marginal error
Therefore adding 10% of non-response rate it was 422
Sampling techniques and procedure
There are 6 public hospitals under Addis Ababa health bur eau from those four hospitals (Tirunesh Beijing General Hospital (TBGH), Zewditu Memorial Hospital (ZMH), Minilk II hospital and Ghandi Memorial hospital) was taken by simple random sampling. After proportional allocation was done, each mother was selected every K interval in each hospital (k for ZMH = 3, GMH =3, TBGH = 3 and MIIH = 3).
Variables
Dependent Variable
• Magnitude of shifting from private to public health fa cilities among pregnant mothers with previous caes arean scars
Independent Variables
• Socio-demographic characteristics: Maternal Age, Oc cupation, Marital Status, Educational level, Household income.
• Experience with Private Health Facilities, Current Experience with Public Health Facilities: Reason for choosing of private facility, Level of satisfaction, Costs of private facility, Having health insurance .
• Reproductive History: Parity, Number of pregnancies,Number of previous cesarean deliveries
• Reason for last cesarean, Experience complications from previous cesarean, Place of previous CS
Operational Definition
• Shifting from private to public health facilities: The movement or transition of pregnant mothers with pre vious C-section scars from private health facilities to public health facilities for antenatal care, delivery, or emergency obstetric services [8]
• Private Health Facilities: Non-governmental health institutions, including clinics, hospitals, and maternity centers, that operate on a for-profit or non-profit basis and provide maternal health services [10]
• Public Health Facilities: Government-owned and operated health institutions, including health centers, primary hospitals, and referral hospitals, that provide maternal health services, often at subsidized or no cost [11]
• Pregnant Mothers with Previous Caesarean Scar: Women who are currently pregnant and have a history of at least one previous Caesarean section delivery [8]
• Magnitude: The proportion or percentage of pregnant mothers with a history of Caesarean section at private health facilities but later shifting to public health facili ties for subsequent care or delivery [12]
Data Collection Procedure and Quality assur ance
Data Collection Procedure
A Pre-tested and interviewer-administered structured questionnaire, was prepared in English and translated to Amharic language was used to collect quantitative data. Twenty-four data collectors were participated to collect the data. Training will give to data collectors for three days. The training was focused on the study objectives, questionnaire and process of data collection. The principal in vestigator and coinvestigators were supervised the data collection process and checked filled questionnaire for consistency and completeness.
Data Quality Assurance
The data was collected by 24 data collectors, all of them are the investigators themselves and prior to the com mencement, data collectors was given orientation by principal investigator on the objectives of the study, meth odology of the study and, on issue of confidentiality of in formation gathered. Pre-test was done on St. Paul Hospi-tal The data collection, application of standard procedures and accuracy of tests was supervised and checked daily for its completeness and consistency through close follow up of the advisor.
Data Management
Each questionnaire was checked for completeness, missing values then was manually clean up on such indi cation. Then coded data was entered on to computer using EPi data version 4.7 and analysis was by SPSS version 26.
Statistical Analysis
The data was double checked and all numerical values calculated by using excel. Principal component analysis was carried out for the reduction of variables involved in the magnitude of shifting from private to public health facilities among pregnant mothers with previous caesarean scars. Descriptive statistics was used to summarize cat egorical variables, whereas mean and standard deviations (SDs) was used to present continuous variables. A logistic regression model was employed to ascertain any signifi cant association between independent variables and de pendent variables.
Ethical Consideration
The research proposal was approved by the ethical clear ance committee of TBGH. Then this formal letter was submitted Addis Ababa research and emergency manage ment directorate and approved. Confidentiality was en sured by making the collected information anonymous and data was put secured and in place.
Plans for Dissemination of Findings
The study could be a tool for designing appropriate strat egy for the Magnitude of shifting from private to public health facilities among pregnant mothers with previous caesarean scars and can be taken as a baseline for other studies related studies. Final findings of the study will be submitted to Addis Ababa Health bureau to each hospital. It will be disseminated through publications, presentations, and also disseminated in AA.
Result
Socio-demographic characteristics of pregnant moth ers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025
Out of 422 study participants 418 respondents participated in this study making a response rate of 99.05%. The mean age of the study subjects were 30.80years (+4.14 SD). The minimum age of the study participants was 21 years and the maximum age was 40 years old.The majority of participants (76.3%) were between the ages of 25 and 34; with 38.3% aged 25-29 and 38.0% aged 30-34. Only 3.1% were 24 or younger, while 20.6% were 35 years or older. Regarding marital status, an over whelming majority (94.7%) were married. A small percent age was divorced (3.6%) or widowed (0.7%), and only 1.0% was single.
Education levels varied, with most participants having a secondary education (57.4%). Over a quarter (27.8%) had a primary education, 13.4% had education above the sec ondary level, and a small minority (1.4%) had no formal education.
In terms of occupation, nearly half of the participants (46.9%) were categorized under “other such as house wife” Governmental employees made up 29.4% of the sample, followed by merchants (17.5%), students (3.8%), and farmers (2.4%).
The income level for most participants (63.4%) fell with in the 10,000 to 20,000 EBR range. Smaller proportions earned 10,000 EBR or less (17.0%) or more than 20,001 EBR (19.6%).
Virtually all participants (98.3%) resided in Addis Ababa (AA), with only 1.7% living outside the city. Finally, most participants (68.4%) reported having a family size larger than 3 persons, while 31.6% had a family size of 3 or fewer persons (Table 1).
| Variables | Variable | Frequency | % |
| ≤ 24 | 13 | 3.1 | |
| Age | 25-29 | 160 | 38.3 |
| 30-34 | 159 | 38 | |
| ≥35 years | 86 | 20.6 | |
| Single | 4 | 1 | |
| Marital status | Married | 396 | 94.7 |
| Divorced | 15 | 3.6 | |
| Widowed | 3 | 0.7 | |
| No education | 6 | 1.4 | |
| Educational status | Primary education | 116 | 27.8 |
| Secondary education | 240 | 57.4 | |
| Above secondary | 56 | 13.4 | |
| Government employee | 123 | 29.4 | |
| Merchant | 73 | 17.5 | |
| Occupation | Farmer | 10 | 2.4 |
| Student | 16 | 3.8 | |
| Other | 196 | 46.9 | |
| ≤10000 EBR | 71 | 17 | |
| Income level | 10000 – 20000 EBR | 265 | 63.4 |
| ≥20001 EBR | 82 | 19.6 | |
| Residence | AA | 411 | 98.3 |
| Out of AA | 7 | 1.7 | |
| Family size | ≤ 3 persons | 132 | 31.6 |
| > 3 persons | 286 | 68.4 |
Table 1: Socio-demographic characteristics of pregnant moth ers with previous caesarean scars attending public hospitals, Ad dis Ababa, Ethiopia, 2025, N = 418
Past Gynaecology and obstetrics related factors
Obstetric history of the mother in their 1st labour
Of the 418 women, the vast majority (83.0%) delivered their first child via Cesarean section (CS), while 17.0% had a spontaneous vaginal delivery (SVD). The birth interval between the first and second pregnancy was most com monly 25-36 months (44.3%), followed closely by intervals of ≤24 months (42.8%). A smaller proportion had intervals of 37-48 months (11.0%) or greater than 48 months (1.9%). Following their first CS, most women (63.9%) did not use any family planning method. Among the 36.1% who did, the implant was the predominant choice (74.8%), followed by oral contraceptives (11.9%), injections (7.9%), Jadel le (3.9%), and the IUCD (1.3%). The first birth occurred primarily in a public health facility (84.4%) rather than a private one (15.6%). Most women had three or fewer preg nancies (86.6%), and the birth outcome of the first delivery was overwhelmingly a live birth (96.7%) (Table 2).
| Variables | Variable | Frequency | % |
| Mode of delivery in their 1st labour | SVD | 71 | 17 |
| CS | 347 | 83 | |
| Birth interval between 1st and second pregnancy in months | ≤ 24 months | 179 | 42.8 |
| 25 – 36 months | 185 | 44.3 | |
| 37 – 48 months | 46 | 11 | |
| > 48 months | 8 | 1.9 | |
| Family planning used after 1st CS | Yes | 151 | 36.1 |
| No | 267 | 63.9 | |
| Types of family planning used | Implanon | 113 | 74.8 |
| Injection | 12 | 7.9 | |
| IUCD | 2 | 1.3 | |
| Jadelle | 6 | 3.9 | |
| OC | 18 | 11.9 | |
| Type of health facilities where the mother gave her 1st birth | Public Health Facility | 353 | 84.4 |
| Private Health Facility | 65 | 15.6 | |
| Gravidity | ≤ 3 | 362 | 86.6 |
| > 3 | 56 | 13.4 | |
| Birth outcome | Live | 404 | 96.7 |
| Dead | 14 | 3.3 |
Table 2: First labour related history of pregnant mothers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025, N = 418
Obstetric history of the mother in their 2nd labour Regarding the mode of delivery, the vast majority of moth ers (197, 75.48%) underwent a Cesarean section (CS) for their second birth, while a smaller proportion (64, 24.52%) had a Spontaneous Vaginal Delivery (SVD). The birth interval between the second and the subsequent preg nancy was also analyzed. More than half of the mothers (143, 54.79%) had an interval of 24 months or less. A long er interval of 25 to 36 months was reported by 97 mothers (37.16%), and only 21 mothers (8.05%) had a birth interval exceeding 36 months.
Concerning family planning practices after the second Cesarean section, a majority of mothers (161, 61.69%) reported using some form of family planning. However, a significant portion (100, 38.31%) did not. Among those who used contraception, the most common method was Implanon, used by 118 mothers (45.21% of all mothers, or 73.29% of users). Other methods were used less frequently: Injectable (INJECT) by 13 mothers (4.98%), Intrauter ine Contraceptive Devices (IUCD) by 14 mothers (5.36%), and Oral Contraceptives (OC) by 16 mothers (6.13%). The data also shows that most second births (232, 88.89%) took place in a Public Health Facility, compared to a small-er number (29, 11.11%) that occurred in a Private Health Facility. Finally, the birth outcome was overwhelmingly positive, with nearly all second births (258, 98.85%) re sulting in a live birth. A very small number of cases (3, 1.14%) resulted in a fetal death (Table 3).
| Variables | Variable | Frequency | % |
| Mode of delivery in their 2nd labour | SVD | 64 | 24.52 |
| CS | 197 | 75.48 | |
| Birth interval between 2nd and the second pregnancy in months | ≤ 24 months | 143 | 54.79 |
| 25 – 36 months | 97 | 37.16 | |
| > 36 months | 21 | 8.05 | |
| Family planning after 2nd CS | Yes | 161 | 61.69 |
| No | 100 | 38.31 | |
| Types of family planning used | Implanon | 118 | 45.21 |
| Inject | 13 | 4.98 | |
| IUCD | 14 | 5.36 | |
| OC | 16 | 6.13 | |
| Type of health facilities where the mother gave her 2nd birth | Public Health Facility | 232 | 88.89 |
| Private Health Facility | 29 | 11.11 | |
| Birth outcome | Live | 258 | 98.85 |
| Dead | 3 | 1.14 |
Table 3: Second labour related history of pregnant mothers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025, N = 261
Obstetric history of the mother in their 3rd labour
Of the 77 mothers included in the study, the mode of de livery for their third labour was nearly evenly split, though Caesarean section (CS) was slightly more common. Spe cifically, 35 women (45.45%) had a spontaneous vaginal delivery (SVD), while 42 women (54.55%) delivered via Caesarean section.
A significant majority of the mothers, 50 women (64.94%), had a short birth interval of 24 months or less. A longer interval of 25 to 36 months was reported by 27 mothers (35.06%). The vast majority of mothers who had a third Caesarean section adopted family planning practices afterward. Out of the total, 63 women (81.82%) reported using contraception following their delivery. In contrast, 14 women (18.18%) did not use any family planning methods after their third CS.
For those who used contraception, the most prevalent method was Implanon, chosen by 43 women (55.84% of family planning users and 68.25% of all users). The inject able method was the second most common, used by 21 women (27.27% of users). Other methods were used less frequently; 6 women (7.79%) used an Intrauterine Contra ceptive Device (IUCD), and 7 women (9.09%) used Oral Contraceptives (OC). All recorded third births in the study, 77 (100%), took place in a Public Health Facility. No births occurred in a Private Health Facility. Furthermore, all third birth outcomes were live births, accounting for 100% of cases, with no recorded stillbirths or early neonatal deaths in the dataset (Table 4).
| Variables | Variable |
Frequency |
% |
| Mode of delivery in their 3rd labour | SVD | 35 | 45.45 |
| CS | 42 | 54.55 | |
| Birth interval between 3rd and the second pregnancy in months | ≤ 24 months | 50 | 64.94 |
| 25 – 36 months | 27 | 35.06 | |
| Family planning used after 3rd CS | Yes | 63 | 81.82 |
| No | 14 | 18.18 | |
| Types of family planning used | Implanon | 43 | 55.84 |
| Injectable | 21 | 27.27 | |
| IUCD | 6 | 7.79 | |
| OC | 7 | 9.09 | |
| Type of health facilities where the mother gave her 3rd birth | Public Health Facility | 77 | 100 |
| Private Health Facility | 0 | 0 | |
| Birth outcome | Live | 77 | 100 |
| Dead | 0 | 0 |
Table 4: Third labour related history of pregnant mothers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025, N = 77
Obstetric history of the mother in their 4th labour
Of 14 mothers, the overwhelming majority, 12 (85.71%), delivered their third child via Cesarean section (CS). In contrast, only 2 mothers (14.29%) had a spontaneous vaginal delivery (SVD). Regarding the birth interval between their second and third pregnancies, more than half of the mothers, 8 women (57.14%), had an interval of 25 to 36 months. A shorter interval of 24 months or less was reported by 6 mothers (42.86%).
Following their third Cesarean section, most mothers adopted family planning methods. Ten women (71.43%) reported using contraception, while four women (28.57%) did not use any family planning.
Among the ten users of contraception, the preferred meth od was Implanon, used by 4 women (40% of users). The Intrauterine Contraceptive Device (IUCD) was the second most common choice, utilized by 3 women (30%). Two women (20%) used Oral Contraceptives (OC), and one woman (10%) used the Injectable method.
All recorded third births for this group, 14 (100%), took place in a Public Health Facility, with no births occurring in a Private Health Facility. Furthermore, the birth outcome for all 14 cases was a live birth, with no recorded stillbirths or early neonatal deaths (Table 5).
| Variables | Variable | Frequency | % |
| Mode of delivery in their 3rd labour | SVD | 2 | 14.29 |
| CS | 12 | 85.71 | |
| Birth interval between 3rd and the second pregnancy in months | ≤ 24 months | 6 | 42.86 |
| 25 - 36 months | 8 | 57.14 | |
| Family planning used after 3rd CS | Yes | 10 | 71.43 |
| No | 4 | 28.57 | |
| Types of family planning used | Implanon | 4 | 40 |
| Injectable | 1 | 10 | |
| IUCD | 3 | 30 | |
| OC | 2 | 20 | |
| Type of health facilities where the mother gave her 3rd birth | Public Health Facility | 14 | 100 |
| Private Health Facility | 0 | 0 | |
| Birth outcome | Live | 14 | 100 |
| Dead | 0 | 0 |
Table 5: Fourth labour related history of pregnant mothers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025, N = 14
Family planning utilized in inter pregnancy vs Grav idity
The highest utilization rate is observed among Gravida III mothers (third pregnancy), with 81.82% reporting “Yes” to using family planning in the inter-pregnancy period. This is followed by Gravida IV and above mothers (fourth or more pregnancies), with a utilization rate of 71.43%. Gravida II mothers (second pregnancy) also show a relatively high utilization rate of 61.69%. In contrast, Gravida I mothers (first pregnancy) have the lowest utilization rate at 36.1%.
Conversely, the data for those who did not utilize family planning (“No”) shows an inverse relationship. Gravida I mothers have the highest percentage (63.9%) not utilizing family planning, which aligns with their low utilization rate. This percentage decreases sharply with higher gravidity, dropping to 38.31% for Gravida II, 18.18% for Gravida III, and 28.57% for Gravida IV and above. It suggests that the likelihood of a mother utilizing family planning between pregnancies increases with the number of pregnancies up to the third, after which it sees a slight decline for mothers with four or more pregnancies. Gravida I mothers are the least likely to use inter-pregnancy family planning (as shown in the figure 1).
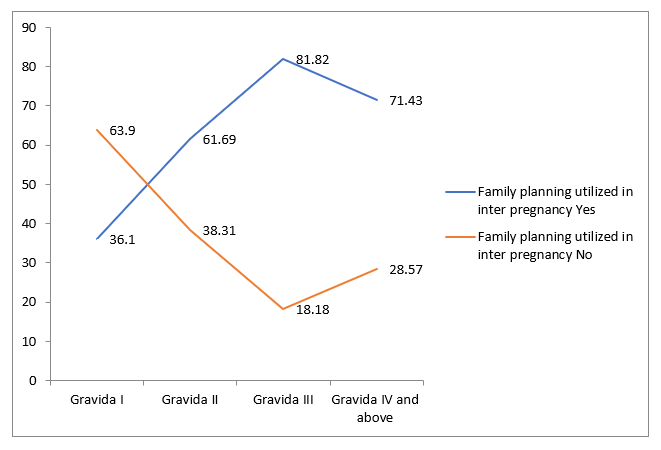
Figure 1: Family planning utilized in inter pregnancy vs Gravid ity of pregnant mothers with previous caesarean scars attending public hospitals, Addis Ababa, Ethiopia, 2025
Scar related history of pregnant mothers with previ ous caesarean scars attending public hospitals
Nearly a quarter of the respondents (23.7%, n=99) re ported having had a Caesarean delivery in a private health facility before, while the vast majority (76.3%, n=319) had not. Among those who had a CS in a private facility, the experience was overwhelmingly a one-time occurrence, with 92.93% (n=92) having had only one CS and a much smaller proportion (7.07%, n=7) having had two. A significant number of women (27.8%, n=116) experi enced complications from a previous caesarean deliv ery, though most (72.2%, n=302) did not report any com plications. The primary reasons for the initial caesarean section were varied. The most common reason was fetal distress, accounting for 33.01% (n=138) of cases. This was followed by “Other” reasons, such as fetal macrosom ia (28.71%, n=120), failed augmentation or induction of labour (17.46%, n=73), maternal request (9.33%, n=39), and fetal malposition & mal presentation (11.48%, n=48). The data clearly shows that public health facilities were the predominant location for the last caesarean delivery, with 86.6% (n=362) of the procedures performed there. In contrast, a small minority (13.4%, n=56) had their last CS performed in a private health facility. This distribution is listed twice in the data, confirming the significant role of public health facilities in providing caesarean section ser vices for this population (table 6).
| Variables | Variable | Frequency | % |
| Did you have CS delivery in private health facilities before | Yes | 99 | 23.7 |
| No | 319 | 76.3 | |
| Frequency of CS delivery in private health facility | Only one time | 92 | 92.93 |
| Two time | 7 | 7.07 | |
| Did you experience complications from previous cesarean | Yes | 116 | 27.8 |
| No | 302 | 72.2 | |
| Primary reason for initial cesarean section | Maternal request | 39 | 9.33 |
| Fetal distress | 138 | 33.01 | |
| Failed augmentation/ induction | 73 | 17.46 | |
| Fetal malposition & mal presentation | 48 | 11.48 | |
| Others (e.g fetal macrosomia) | 120 | 28.71 | |
| Where was your last cesarean performed? | private HF | 56 | 13.4 |
| public health facility | 362 | 86.6 | |
| Where was your last cesarean performed? | private HF | 56 | 13.4 |
| public health facility | 362 | 86.6 |
Table 6: Scar related history of pregnant mothers with previous caesarean scars attending public hospitals
Magnitude of shifting from private to public health fa cilities
The analysis reveals that 23.7% (n=99) of the total 418 re spondents had a history of Cesarean section (CS) delivery in a private health facility before shifting to a public facility for their current care. This proportion has a 95% confi dence interval ranging from 19.4% to 27.8% (Figure 2).
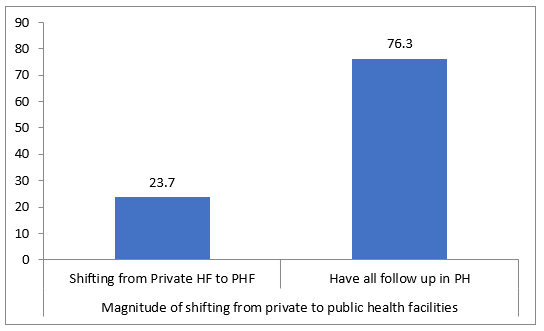
Figure 2: Magnitude of shifting from private to public health facilities of pregnant mothers with previous caesarean scars at tending public hospitals, Addis Ababa, Ethiopia, 2025
Conversely, the vast majority of women, 76.3% (n=319), reported having all of their follow-up care conducted with in the public health system from the outset, with no prior history of private facility CS delivery. The 95% confidence interval for this group is 72.2% to 80.6%.
This data indicates a clear pattern of patient movement within the healthcare system. While a substantial major ity consistently use public health services for their obstet ric care, a defined minority—approximately one in four women—transition from the private sector to the public sector. The narrow confidence intervals around these es timates provide a robust measure of precision, suggesting the sample provides a reliable reflection of this behavior in the broader population. This shifting could be influenced by various factors such as cost, perceived quality of care, insurance status, or complications in previous pregnan cies.
History of current pregnancy of pregnant mothers with previous caesarean scars
Based on the provided data, the majority of current preg nancy referrals (89.7%) were made to government health facilities, while a smaller proportion (10.3%) were to pri vate health facilities. Regarding previous cesarean sec tions, most mothers (62.4%) had a history of two or more CS scars, while 37.6% had one CS scar. For those with a single scar, the planned mode of delivery for the current pregnancy was predominantly a repeat Cesarean Sec tion (78.34%), followed by a Trial of Labor After Cesarean (TOLAC) (15.29%); a small percentage (6.37%) had not yet decided.
The gestational age (GA) of the current pregnancies was most commonly between 36+1 and 40 complete weeks (85.9%). Smaller proportions were at 32+1 to 36 weeks (6.2%), more than 40 weeks (4.1%), and 28 to 32 weeks (3.8%). A majority of respondents (62.4%) reported experiencing challenges, with the most significant issue being long waits (88.9% of those who faced challenges). Other challenges included staff attitude (10.3%) and resource shortages (0.8%) (Table 7).
| Variables | Variable | Frequency | % |
| Place of current pregnancy referral | Government health facilities | 375 | 89.7 |
| Private health facility | 43 | 10.3 | |
| Number of PCS the mother have | 1PCS scare | 157 | 37.6 |
| 2 and above CS scar | 261 | 62.4 | |
| Plan for mode of delivery for the current pregnancy (those who have one scar) | CS | 123 | 78.34 |
| TOLAC | 24 | 15.29 | |
| Not decided | 10 | 6.37 | |
| GA of current pregnancy | 28 - 32 complete weeks | 16 | 3.8 |
| 32+1 - 36 complete weeks | 26 | 6.2 | |
| 36+1 - 40 complete weeks | 359 | 85.9 | |
| > 40 weeks | 17 | 4.1 | |
| Did you experience any challenges here | Yes | 261 | 62.4 |
| No | 157 | 37.6 | |
| What was the challenge | Long waits | 232 | 88.9 |
| Staff attitude | 27 | 10.3 | |
| Resource shortages | 2 | 0.8 |
Table 7: History of current pregnancy of pregnant mothers with previous caesarean scars attending antenatal car at Addis Ababa Public hospital, 2025
Previous Experience with Private Health Facilities and reasons of shifting
Based on the data provided, the primary reason patients initially chose a private healthcare facility was a perceived better quality of care, cited by 21.8% of respondents. This was followed by referrals (16.7%) and shorter wait times (15.1%). The decision to switch from a private to a public facility was made by the vast majority (74.8%) during pregnancy, rather than before (25.3%). An overwhelming 91.9% reported that cost was a barrier to continuing care at the private facility.
When deciding to switch, over half of the respondents (56.6%) were assisted by their family, while a significant portion (15.2%) reported having no help. Most patients (89.9%) were unaware of the professional scope of the surgeon who performed their prior surgery in the private facility. Regarding the estimated cost of their last Caesarean section, the majority (54.6%) paid between 20,000 and 40,000 ETB, with 31.3% paying more than 40,000 ETB and 14.1% paying less than 20,000 ETB (Table 8).
| Variables | Variable | Frequency | % |
| Why did you initially choose a private facility? | Perceived better quality | 57 | 57.6 |
| Self-referral | 10 | 10.1 | |
| Shorter wait times | 12 | 12.1 | |
| Other | 20 | 20.2 | |
| When did you decide to switch to a public facility? | Before pregnancy | 25 | 25.3 |
| During pregnancy | 74 | 74.8 | |
| Were costs a barrier in the private facility? | Yes | 91 | 91.9 |
| No | 8 | 8 | |
| Who help you before switching? | Health worker | 12 | 12.1 |
| Family | 56 | 56.6 | |
| Friends | 11 | 11.1 | |
| No one | 15 | 15.2 | |
| Others reason | 5 | 5 | |
| Did you know the professional scope of the surgeon did your surgery in private health facility? | Yes | 10 | 10.1 |
| No | 89 | 89.9 | |
| Estimated cost paid for the last CS (ETB): | < 20,000 EBR | 14 | 14.1 |
| 20,000 -40000 EBR | 54 | 54.6 | |
| > 40,000 EBR | 31 | 31.3 |
Table 8: Previous Experience with Private Health Facilities and reasons of shifting of pregnant mothers with previous caesarean scars attending antenatal car at Addis Ababa Public hospital, 2025
Factors associated with shifted from private to public health facilities for delivery care
In bivariable analysis those who have a family size (> 3 per sons) 3.564(1.938 – 6.555), Family income 5.864(2.492 - 11.802), age (≥35 years) 5.763 (3.531- 9.023), Cost paid for private HF (2000 br and below) 4.167(1.053 - 16.484), Educational status (above secondary) 4.108(2.009 –9.903), Occupational status (Governmental employee) 2.152(1.309–8.645) were candidate for multivariable an alysis. But GA, place of current referral and marital status were lost their significance.
In multivariable analysis, those predictors which showed statistical significance in bivariable analysis and p value less than 0.2 were used to run multivariable analysis. Par ticipants who have family size 3 and more were about 4 times more likely shifted from private to public health facili ties for delivery care as compared to those whose family size is below 3 (AOR= 3.564: CI= 2.432 – 8.432). Those participants whose family income 10,000Br and below were about five times more likely to shift from private pub lic health facilities as compared to those who get a family income 20001 Br and above AOR = 4.728: CI= 2.843 – 9.392). Participants aged 35 years and above had signifi cantly higher odds of making this shift compared to their younger counterparts (AOR = 3.20; 95% CI: 2.10, 8.11). Individuals with an education level above secondary had significantly higher odds of making this shift compared to those with a secondary education or less (AOR = 5.23; 95% CI: 2.04 – 11.30) (as shown in table 9).
| Variable | Shifting from private to public health facilities | 95% CI | P Value | |||
| Yes | No | COR | AOR | |||
| Family size | ≤3 | 85 | 201 | 1 | 1 | |
| > 3 | 14 | 118 | 3.564(1.938 – 6.555)* | 3.564(2.432 – 8.432)** | 0.01 | |
| Family income | ≤10000Br | 8 | 63 | 5.864(2.492 - 11.802)* | 4.728(2.843 – 9.392)** | 0.00 |
| 10000 – 20000 Br | 56 | 209 | 2.779 (1.640 - 4.711) | 3.934(1.923 – 7.437) | ||
| ≥20001 Br. | 35 | 47 | 1 | 1 | ||
| Age | ≤24 years | 5 | 8 | 1 | 1 | |
| 25 - 29 years | 51 | 109 | 4.103(2.592 – 10.002) | 5.320 (3.031- 10.318) | ||
| 30 - 34 years | 36 | 123 | 2.002(1.421 – 8.841) | 3.432(2.062- 7.102) | ||
| ≥35 years | 7 | 79 | 5.763 (3.531- 9.023)* | 3.201(2.101– 8.105)** | 0.00 | |
| Cost paid | <20000 | 7 | 7 | 4.167(1.053 - 16.484) | 4.198(3.105 - 7.901) | |
| 20000 - 40000 | 44 | 10 | 0.947(0.307 - 2.917) | 3.930(2.221 – 5.054) | ||
| >40000 | 25 | 6 | 1 | 1 | ||
| Educational status | No education | 0 | 6 | 1 | 1 | |
| Primary education | 16 | 100 | 0.893 (0.345 - 0.993) | 5.194(1.002 – 9.005) | ||
| Secondary education | 76 | 164 | 3.640(1.221 – 8.054) | 4.009(3.0103– 8.001) | ||
| Above secondary | 7 | 49 | 4.108(2.009 – 9.903)* | 5.230(2.038– 11.302)** | 0.00 | |
| Occupational status | Governmental employee | 25 | 98 | 2.152(1.309–8.645) | 1.108(1.000 – 8.104) | |
| Merchant | 25 | 48 | 6.108(3.028 – 12.038) | 4.204(8.302 – 14.038) | ||
| Farmer | 0 | 10 | 2.424(1.009-10.030) | 4.005(2.038– 9.001) | ||
| Student | 8 | 8 | 3.040(1.002–6.022) | 4.920(2.003– 8.305) | ||
| Other | 41 | 155 | 4.043(2.092– 8.604) | 4.532(2.085– 8.097) | ||
| *Statically significance in bivariable analysis, ** statically significance in multivariable analysis | ||||||
Table 9: Bivariate and multivariate analysis of shifting of pregnant mothers with previous caesarean scars attending antenatal car at Addis Ababa Public hospital, 2025
Discussion
This study aimed to identify factors associated with the shift from private to public health facilities for delivery care among women in Addis Ababa. The level of shifting of pregnant women with history previous CS from private to government health facilities and it reveals that 23.7% (n=99) with a 95% confidence interval ranging from 19.4% to 27.8% of the total 418 respondents had a history of Cesarean section (CS) delivery in a private health facility before shifting to a public facility for their current care.
Globally, in low and middle-income countries (LMICs) facing high out-of-pocket expenditures, similar shifting patterns are pronounced; for instance, a study in Sub-Sa haran Africa countries reported a much higher magnitude, where 62% of women who had a previous CS in a private facility sought subsequent care in the public sector, pri marily driven by cost [13].
The findings reveal that larger family size, lower family income, advanced maternal age, and higher educational attainment are significant predictors of this shift. The dis cussion contextualizes these findings within the broad er landscape of maternal healthcare seeking behaviour, moving from global perspectives to the specific socio-eco nomic realities of Addis Ababa.
This study aimed to identify factors associated with the shift from private to public health facilities for delivery care among women in Addis Ababa. The findings reveal that larger family size, lower family income, advanced maternal age, and higher educational attainment are significant predictors of this shift. The discussion contextualizes these findings within the broader landscape of maternal health care seeking behaviour, moving from global perspectives to the specific socio-economic realities of Addis Ababa.
The strongest predictor identified was low family income (≤10,000 Br), which increased the odds of shifting to pub lic facilities by nearly five times which is corroborated by multiple other investigations across different contexts. For instance, a study in Nepal found that households in the lowest income quintile were 4.8 times more likely to use public health facilities compared to those in the highest quintile, a finding nearly identical to the near five-fold in crease in odds reported here [14]. Similarly, research in Bangladesh demonstrated that economic constraints were a primary driver for choosing public hospitals, with cost being a more significant factor than quality of care for low-income households [15]. This pattern is further sup ported by a systematic review which concluded that catas trophic health expenditures often force poorer families to seek more affordable care in the public sector, even when preferences might lie elsewhere [12]. These consistent findings highlight how financial barriers profoundly shape healthcare-seeking behaviour, consistently making low income a dominant predictor of reliance on public health services across various settings.
At a national level in Ethiopia, this is strongly supported by the government’s push for universal health coverage (UHC) through the expansion of primary healthcare and the removal of user fees for maternal services in public facilities. Studies from other Ethiopian regions have con sistently shown that financial constraints are a primary bar rier to utilizing private health services [3]. The finding from Addis Ababa, 2025 underscores that even in the capital city, where private facilities are more prevalent, economic vulnerability remains a decisive factor. As the cost of living in Addis Ababa continues to rise, families with stagnant in comes are likely reallocating limited resources, choosing the free or subsidized delivery services in public hospitals despite potential concerns about quality or crowding.
Participants with a family size of three or more were about four times more likely to shift to public facilities. This can be interpreted through a life-course and economic lens. Globally, as families expand household expenses multiply, necessitating more prudent financial management. A de livery in a private facility represents a significant, one-time cost that becomes increasingly difficult to justify when re sources must be spread across more dependents [4].
Furthermore, the significantly higher odds (AOR=3.20) among women aged 35 years and above align with this life-stage explanation. Older mothers are more likely to have larger families and may be facing concurrent finan cial pressures, such as educational expenses for older children. They may also possess more experience with the healthcare system, leading to a pragmatic decision to utilize a known, cost-effective public service for a rou tine delivery, especially if their previous pregnancies were uncomplicated. This contrasts with younger, first-time mothers who might prioritize perceived comfort and indi vidualized attention in a private facility.
A particularly intriguing finding is that women with an edu cation level above secondary had over five times higher odds of shifting to the public sector. This ap pears counterintuitive, as global literature often associates higher education with greater health literacy and a prefer ence for higher-quality care, typically sought in the private sector [5]. However, in the specific context of Addis Ababa, this finding can be explained by several factors.
Firstly, higher education likely correlates with better know ledge of the Ethiopian government’s flagship health pro grams, such as the Health Extension Program and the net work of public hospitals. Educated women may be more aware of the improved capabilities and specialized servi ces available in leading public hospitals like Tikur Anbesa or St. Paul’s. Secondly, they may make a more calculated, informed trade-off, choosing to save substantial financial resources for postnatal and child-rearing expenses by opt ing for a free public delivery. This reflects a strategic allo cation of household resources based on long-term plan ning rather than a simple preference for private care. This nuanced decision-making by educated women has been observed in other LMIC urban settings, where the quality gap between top-tier public and mid-range private facilities is narrowing [6].
The confluence of these factors paints a clear picture of the evolving maternal healthcare landscape in Addis Ababa. The shift from private to public facilities is not merely a de fault option for the poor but a conscious, strategic choice for a growing segment of the urban population, including older, more educated women with larger families. This trend suggests a possible increasing confidence in the public health system’s ability to handle normal deliveries. However, it also raises critical questions for policymakers. This influx of patients with potentially higher expectations could strain the already overburdened public hospitals, potentially impacting the quality of care and waiting times.
Recommendation for Stakeholders
The summary of recommendations to manage the shift of patients from private to public health facilities in Addis Ababa is structured across four key stakeholders. The Addis Ababa Regional Health Bureau (AARHB) should focus on systemic solutions, including introducing a tar geted health subsidy for low-income families and a rapid public capacity expansion to relieve strain on public hos pitals. Public Hospitals are advised to manage the influx by improving operational efficiency, such as establishing dedicated Low-Risk Delivery Units (LRDUs) for routine cases and improving the non-clinical aspects of care like privacy and communication to meet the expectations of educated patients. Private Health Facilities are primarily encouraged to address cost barriers by introducing bun dled, fixed-price maternity packages and developing CSR discount programs for larger, lower-income families. Final ly, Healthcare Professionals (HCPs) across both sectors should be trained to adopt a “Financial Reality” counsel ling approach to proactively discuss cost-benefit trade-offs with patients and improve inter-facility communication for seamless and safe care, particularly for high-risk patients.
Strength and limitation of the study
The study possesses significant strengths, primarily its focus on the high-risk population of pregnant women with a previous Cesarean Section (CS), providing robust quantitative evidence of the magnitude of the patient shift (23.7%) and identifying strong predictors like the nearly five-fold increased odds of shifting due to low family income. Furthermore, it offers a nuanced contextual inter pretation that re-frames the finding of higher educational attainment as a predictor, suggesting a strategic alloca tion of resources by informed women, making the findings highly policy relevant for Addis Ababa’s health systems. However, the study is subject to several limitations, includ ing a potential selection bias as it only included women who had already shifted to public facilities, which limits the generalizability of the predictor findings. Additionally, the research lacked a quantitative public quality metric to measure the actual impact of the patient influx on quality of care or waiting times in public hospitals, and it provided limited exploration of the prior CS experience in the private sector, failing to deeply investigate how specific details of that care might have influenced the subsequent decision to shift.
Conclusion
This study examines the determinants influencing preg nant women in Addis Ababa to transition from private to public health facilities for delivery care. Key findings indicate that economic vulnerability, primarily tied to low family income, significantly increases the likelihood of this shift. Additional factors such as larger family sizes and advanced maternal age further necessitate careful finan cial planning. Interestingly, higher educational attainment correlates with this shift, suggesting that educated women strategically choose public services for cost-saving bene fits. This trend challenges the common perception that such shifts are solely indicative of poverty; instead, it re flects informed decision-making in healthcare. The public sector’s rising patient volume, including those with prior Cesarean sections, raises concerns regarding quality of care and demands innovative solutions from policymakers and private facilities, such as targeted subsidies and fixed price delivery packages. Addressing these shifts requires recognition of underlying socio-economic complexities to balance quality and access in maternal care.
Abbreviations
ANC Antenatal care
AARHB Addis Ababa Regional Health bureau
AOR Adjusted Odds Ration
COR Crude Odds Ratio
CS Caesarean sections
EDHS Ethiopian demographic and health survey
GMH Ghandi Memorial hospital
HEP Health Extension Program
LMICs Low- and middle-income countries
MIIH Minilk II hospital
MMR Maternal mortality ratio
NGO Nongovernmental organization
SDGs Sustainable Development Goals
TBGH Tirunesh Beijing General Hospital
WHO World Health Organization
ZMH Zewditu Memorial Hospital
Declaration
Ethical approval and consent to participate
Ethical approval and clearance were obtained from re search and ethical committee of Tirunesh Beijing Gen eral Hospital and Addis Ababa research and emergency management directorate Institutional Review Board. In formed written consent was obtained from all study par ticipants. Participants were informed about the objective of the study. After information is provided about purpose of the study, confidentiality of the information and all the par ticipants were reassured of the anonymous (unnamed), and as personal identifiers was not used.
Availability of data and materials
All data included in this manuscript can be accessed from the corresponding author upon request through the email address.
Competing interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publica tion of this article.
Consent for publication
Not applicable
Funding
The author(s) received no financial support for the re search, authorship, and/or publication of this article.
Acknowledgement
We would like to express our great appreciation to GOD. In addition, we would like to express our Special gratitude goes to Tirunesh Beijing General Hospital and Research and training department as well as ethical review committee. Again, we would like to extend our deepest thanks to our beloved parents.
References