Getahun EB1*, Tenaw EK2
1Department of Research and Training, Tirunesh Beijing General Hospital, Addis Ababa, Ethiopia
2General public health at Addis Ababa Reginal Health Bureau, Ethiopia
*Correspondence: Enyew Belay Getahun, Department of Research and Training, Tirunesh Beijing Hospital, Addis Ababa, Ethiopia, Email: enyewadress@gmail.com ORCID: https://orcid.org/0000-0001-6792-2470
Received: 12 Sept, 2025; Accepted: 06 Oct, 2025; Published: 14 Oct, 2025 .
Citation: Getahun EB and Tenaw EK. “Maternal Satisfaction with Delivery Service and Associated Factor Among Post Partum Women at Addis Ababa Public Hospitals, Addis Ababa, Ethiopia 2024.” J Gynecol Matern Health (2025): 116. DOI: 10.59462/3068-3696.3.1.116
Copyright: © 2025 Enyew Belay Getahun. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Abstract
Background: WHO recommends respectful, women centered maternity practices and regular evaluation of women’s satisfaction with care, while Ethiopia’s free maternal healthcare policy addresses pregnancy related mortality. Reports in Addis Ababa, public hospitals special focused on maternity care service showed that there are high number of self-referrals which indicate women are not preference to give birth in Public hospitals which might be less satisfaction by public hospital service. The aim of this study is to assess maternal satisfaction with delivery service and associated factor among post-partum women at public hospital Addis Ababa Ethiopia 2024 G.C
Methods: A facility based cross sectional study design was conducted from May to June 2024 in Addis Ababa public hospitals. Four hospitals were selected randomly and then Systematic random sampling technique was used to select 394 mothers who will give birth within the study period. The data was collected at labor ward. The satisfaction of mothers was measured using 27 questions that were adopted from different literatures. Bivariable and Multivariable logistic regression was fitted to identify independent predictors of maternal satisfaction. The collected data was entered into the Epi Info version 3.1 software and then was exported to SPSS Version 26 for analysis. Those variables whose p value less than 0.2 in Bivariable logistic regression was candidate for multivariable analysis and those variables whose p value less than 0.05 was considered as significant to maternal satisfaction.
Result: Out of 394 study participants 390 respondents participated in this study making a response rate of 98.99%. The overall maternal satisfaction with the delivery service was 221 (56.7%) with (C.I of 51.5 - 60.8). Those participants who delivered without complication AOR =7.177 (CI: 4.761-9.698), those participants who had 4 ANC visits, participants who get an income of 5000 and above were about 2 times more satisfied as compared to their counter parts AOR = 2.02(CI:1.25-3.26)
Conclusion: The finding of this study is revealing a satisfaction rate is low. Strengthening ANC follow up is recommended, maximizing their income should be recommended. Health education and counseling of those mothers to have close ANC follow up
Keywords: Maternal, Satisfaction, Delivery Service, Post-Partum, Public, Hospital
Introduction
Background of the study
Satisfaction with delivery care services is a means of secondary prevention of maternal mortality, since satisfied women may be more likely to adhere to healthcare providers’ recommendations. Satisfaction is defined as the state of pleasure or contentment with an action, event or service and is determined by clients’ expectations and experiences [1]. Maternal satisfaction with the services provided during delivery has been recognized as a critical indicator of the quality of a healthcare system. Satisfied clients have a higher chance of returning to the facility in the future and of recommending the institution to their neighbours and relatives [2].
Since contented women are more likely to follow medical professionals’ advice, satisfaction with delivery care services is a strategy for secondary prevention of maternal death. Client expectations and experiences impact what constitutes satisfaction, which is described as a feeling of pleasure or happiness with an activity, event, or service [1]. Globally, more than 830 women died within a day with cases related to pregnancy and childbirth problems, in 2017 [1]. Of which, 99% of the death is happened in developing country and 66%in sub-Saharan Africa nations. In 2015, 216 maternal deaths per 100, 000 live births were estimated globally. Of these, more than half had occurred in Africa [3]. In Ethiopia, the magnitude of maternal mortality is very high and one of the most crucial problems of the country [3].
In 2016, the number of maternal mortality in Ethiopia was 416 from 100,000 live births and its neonatal mortality was 27 from 1000 new born [3]. In 2015, 216 maternal deaths per 100, 000 live births was estimated globally. Of these, more than half had occurred in Africa [2]. In Ethiopia, the magnitude of maternal mortality is very high and one of the most crucial problems of the country [3]. In 2016, the number of maternal mortality in Ethiopia was 416 from 100,000 live birth and its neonatal mortality was 27 from 1000 new born [1].
Improving maternal health is one of the eight Millennium Development Goals (MDGs) adopted by the international community in 2000 [4]. Under MDG, five countries committed to reducing maternal mortality by three quarters between 1990 and 2015, and Ethiopia is one of those countries [5]. In Ethiopia, maternal mortality has been reduced substantially from 1067 to 416per 100,000 births in 2000 and 2016 and skilled birth attendant coverage rate increased from 60% in 2014/15 to 72.7% 2015/16 [2,3]. As reduction of maternal mortality is one of the sustainable development goal that will end in 2030, Ethiopia is expected to reduce maternal mortality ratio (MMR) from 416 per 100 000 live births in 2016 to 199 per 100 000 live births by 2030. The World Health Organization promotes skilled attendance at every birth to reduce maternal mortality and recommends that women ‘s satisfaction be assessed to improve the quality of health care [4]. In order to improve maternal health care services, maternal satisfaction with care provided be needs to be assessed for appropriate intervention [8]. Every women labor and delivery experience has unique sensitivity to environmental factors [8]. Moreover, events and the interactions occurring during labor have powerful psychological effects. Therefore, a positive childbirth experience is desirable for the benefit of both the parturient woman and her child [8]. Maternal satisfaction has been widely recognized as one of the indicators of the quality and the efficiency of the health care systems [8]. Several studies was conducted on maternal satisfaction assessment in different parts of the world with differences of maternal satisfaction across continents, countries, and health facilities.
A study done in Pakistan and South Australia indicated that the level of maternal satisfaction on delivery care was 61% and 86.1%, respectively [9,10]. However, the studies on the level of satisfaction of mothers in African countries found that only 56% and 51.9% of mothers was satisfied with delivery services in Kenya and south Africa, respectively [11,12].
World Health Organization recommends that there should be monitoring and evaluation of maternal satisfaction in health care institutions to improve the quality and efficiency of health care during pregnancy, childbirth, and puerperium [7]. In Ethiopia, maternal satisfaction studies was conducted in different hospitals. The studies carried out in Amhara Referral Hospitals and Assela Hospital revealed that mother’s satisfaction was 61.9% and 80.7% on delivery services, respectively [13]. From the studies, the factors influencing the satisfaction level have also been evaluated from structural, process and outcome dimension as well as there are other factors which determined maternal satisfaction [17].
Statement of the Problem
The World Health Organization (WHO) also recommended thoughtful, women-centered, and evidence-based maternity practices to improve the outcomes of delivery services. It also suggests routinely evaluating women’s satisfaction with the care they get [12]. In Ethiopia, the government has implemented a free maternal healthcare policy to reduce pregnancy-related mortality. However, maternal satisfaction with delivery services is still a serious concern [16, 2]. Despite the implementation of compassionate, respectful and caring health services by the Ethiopian Federal Ministry of Health, the level of maternal satisfaction with delivery services at public hospitals remains poorly addressed [8].
Suboptimal maternal health services negatively impact health outcomes and public health. High patient satisfaction is a key indicator of quality health service, as it increases willingness to return to health institutions, recommends to family and friends, and reduces maternal mortality due to lack of follow-up, home delivery, and delayed health institution arrival [20,21]
Despite the implementation of compassionate, respectful and caring health services by the Ethiopian Federal Ministry of Health, the level of maternal satisfaction with delivery services at public hospitals remains poorly addressed. In Ethiopia, women do not have confidence in the quality of public hospital services. However, little is known about maternal satisfaction; almost all previous studies are either qualitative studies or measure satisfaction levels using a simple yes/no questionnaire [12,13] in which predictors are not well addressed. Therefore, this study tried to overcome this gap. Thus, it aimed to assess maternal satisfaction with delivery care services at public health hospitals in Addis Ababa, Ethiopia.
Significance of the study
The finding of this study will assess maternal satisfaction with maternity services and it helps for policy makers designing programs and quality improvement projects that improve maternal health services. It can also provide systematic information for service providers, local planners, and other stakeholders to understand how well the delivery service is performing according to client perceptions and what changes may be needed to meet client preferences.
Therefore, this study aims to assess the level of maternal satisfaction on delivery care services provided at public hospitals and factors affecting the maternal satisfaction that will help to fill knowledge gaps in the study area.
Literature Review
Introduction
In 1990s researchers, health policy-makers and managers gave more attention to the patient perception of the quality of health services argued and developed well designed questionnaires allow to assess both the technical competence and interpersonal skills of health professionals [29]. Patients feedbacks are essential in order to measure performance and to make healthcare professionals more aware of aspects enhancing user’s satisfaction. Specially, looking at the patient characteristics as well as the contextual elements that more influence the patient experience can be helpful in order to better identify the service area to be improved [29].
Studies revealed the presence of several factors that influence the level of maternal satisfaction which include structural, process, outcome elements [17]. And also, Socio-demographic status, cost of the service and obstetric history of mother also the other are factor for maternal satisfaction [17].
Maternal satisfaction with delivery services
Maternal Satisfaction is a multidimensional construct involving interpersonal manner, quality of care, accessibility or convenience, finance of care, consistency, physical environment and availability of drug and medical supplies [16]. Overall satisfaction of mothers is concerned with the maternity services as a whole offered to the women. The Studies in Pakistan and South Australia founded that maternal satisfaction was 61% and 86.1% respectively. Similarly, studies conducted in Nairobi, Senegal, and Serbian public hospital the overall level of maternal satisfaction on delivery care was 56%, 88.4%and 82.5%, respectively [11,32,33]. A study conducted in Nigeria referral hospital, few of the participants expressed satisfaction with the quality of care they received during antenatal, intra- partum, and postnatal care [34].
Many had areas of dissatisfaction, or was not satisfied at all with the quality of care [34]. According to a study in Debre markos and Ha was a hospital the overall satisfaction level of mothers with delivery services was 82% and 87.7℅respectively [35,36]. And another study from Amhara region referral and Bahirdar Felege Hiwot hospital overall satisfaction level on delivery service was found to be only 61.9 % and 75 % [13,37]. A recent study conducted in St Paul ‘s millennium hospital in Addis Ababa the level of overall maternal satisfaction on delivery service was 19% [15].
Mothers’ satisfaction with delivery service and associated factors
Studies conducted in different countries to understand determinants of maternal satisfaction have identified various factors influencing health service use. These factors can be categorized as, all across structure, process and outcome. Additionally, socio-economic status, cost of care, obstetric history of mother and demographic factor contribute to maternal satisfaction [17]. The expected relation between the independent and dependent variables is depicted pictorially in the conceptual framework below following the detail discussion of these factors.
Structure
Structure measures assess the infrastructure of health care settings, including facilities, personnel, drug and medical supplies and/or policies related to care delivery [31]
Physical environment
Comfortable physical environment and good administration set up are important predictor in women ‘s positive Assessment of the health facility and maternal care services. Those are all infrastructure in the facility which including access to drinking water, latrine, hand- was hing facility, access of toilet and availability of waiting area, room space, overcrowding environment, silence of the delivery room, availability of maternal waiting room, distance(access) of the facility etc.) [18]. The study conducted in Nepal showed overcrowding increased the likelihood of dissatisfaction, and this study suggested that health facilities should be improve, re-organization of services to eliminate delays [20]. Similarly, the study conducts in Iran showed regarding the environmental factors, the lowest satisfaction was related to respecting silence in the pain room (69.5%) [38].
Similarly, the studies conducted in Amhara, Assela and, Mekele referral hospital maternal satisfaction influenced by access to drinking water, latrine, hand washing facility, access of toilet and availability of waiting area [13,14,27], and also the study conducted in west Gojjam zone, a t Bure town showed welcoming hospital environment was independent predictors for maternal satisfaction [39]. Those clients who consider the hospital as welcoming environment was 3.09 times more likely to satisfy with maternal service [39]. The Study in Jimma showed from Mothers who used MWH (Maternal waiting home) service prior to their delivery had 96% increased satisfaction, compared to those did not used the service and mothers admitted to MWH 87(87.0%) of them will recommend their friends or relatives to use the service in the future [40].
Cleanliness of Health facility
Most Studies showed, over all cleanliness of health institution, particularly labor and delivery room cleanness are the most determinants factor for maternal satisfaction on delivery service. These include cleanliness of delivery room and ward, toilet, showier room, hand wash room, etc. [18]. The Studies conducted in South Africa, Iran (84%), and Kenya was showed cleanliness toilet and hygiene of the delivery room was found important structural factors affecting of maternal satisfaction [12,41]. And also, in Ethiopia, the study conducted in Assela cleanliness of toilet during delivery service was also significant predictor of satisfaction, and dissatisfaction was reported to be highest (42.3%) by cleanliness and access of toilet [14]. Additionally, studies conducted in Gandhi, Mekele, Debre markos hospital and Jimma public health facilities zone mothers was dissatisfied by cleanliness of delivery room and toilet [16,27,35,40].
Availability of medicines, supplies and services
Availability of prescription drugs, essential equipment like blood pressure monitors or thermometers, lab services and emergency supplies like blood and transfusion services, was reported as significant predictors of satisfaction. [9].
According to the study conducted in Pakistan women was less satisfied by availability of equipment required for complete medical checkup, and also study in Kenya Mothers benefiting from the free delivery services was satisfied with drug and supplies availability (>56%) [9,41].
Availability and adequacy of human resources
Availability and adequacy health worker was found the one predictor of maternal satisfaction. According to the study in Nigeria, the absence of trained health workers was to be the most determinant of dissatisfied with mother [34]. And also, the study conducted in Kenya mothers who benefiting from the free delivery services was satisfied by staff availability in the delivery rooms, availability of staff in the wards (>56%) [41].
Health institution Process
The process of care is dominated determinant factor of maternal satisfaction those include provider behavior in terms of courtesy and non -abuse, privacy, other aspect of interpersonal behavior includes communication, staff confidence, and competence and encouragement to laboring, respectful care and emotional support, pain management [18].
Outcome
Evaluates maternal and neonate condition after received health care service this means maternal satisfaction depend on their immediate condition [31]. The Study on Amhara referral hospital Women ‘s satisfaction with delivery care was associated with immediate maternal condition after delivery.
Financial /cost of care
In Ethiopia, study in Amhara referral hospital cost incurred for service to be associated with mothers ‘dissatisfaction [13]. Similarly, study done in Gamo Gofa zone women who had paid for the services less satisfied than women ‘s who not paid for the service [44].
Obstetric History of Women
In Ethiopia, the studies conducted on Jimma, Felege Hiwot Hospital showed ANC attendance (follow up), and women who have more frequency of visit for delivery service was significant predicators of mother’s satisfaction with the service [40,37]. On other study, in Debere Markos showed women ‘s who having plan to deliver at health institution three times more satisfied than women ‘s who not have plan, and also this study showed mode of delivery are independent predictors of maternal satisfaction [35].
Socio Economic and Demographic Status
The Study conducted at Nepal showed that respondents from hill districts and rural areas was more likely to be satisfied in comparison to respondents from mountain, terrain and urban areas [20].
Accordingly, Study, in Felege Hiwot hospital at Bahirdar showed age of women was important predictors of level of satisfaction [37]. Similarly, studies conducted at Wolaita showed that middle aged 20-34 postpartum mothers was more likely to be satisfied when compared to their 35-49 counter age groups where the later might have no/wrong experience with the delivery service. Mothers with high school education 9-12 was at higher chance to be satisfied with the service in comparison with higher level of education as it might show higher demand of the more educated group or there may be underestimation of safe delivery.
Conceptual frame work
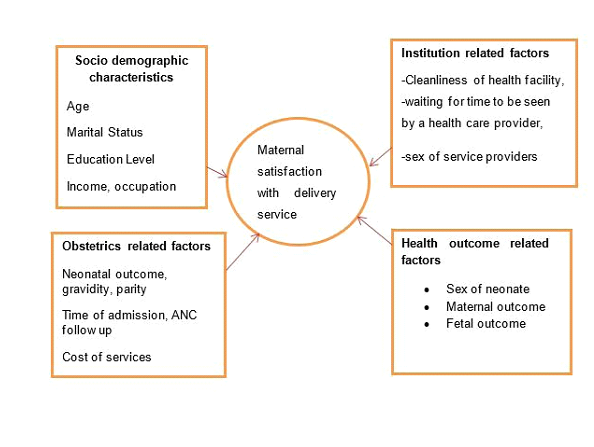
Figure 1. Conceptual Frame Work to assess maternal satisfaction with delivery service and associated factor among post-partum women at public hospital Addis Ababa Ethiopia 2024 G.C(1–4, 9, 15)
Objective
General objective
To assess maternal satisfaction with delivery service and associated factor among post-partum women at public hospital Addis Ababa Ethiopia 2024.
Specific objective
• To assess the magnitude of maternal satisfaction with delivery service among post-partum women at public hospital Addis Ababa Ethiopia 2024.
• To identify factors affecting maternal satisfaction with delivery service among post-partum women at public hospital Addis Ababa Ethiopia 2024.
Methods and materials
Study area
The study was conducted in Addis Ababa’s public hospitals. The city has a population density of 5,535.8 inhabitants per square kilometer and occupies an estimated area of 174.4 square kilometers. In Addis Ababa city administration there are 6 hospitals, 1 Public health laboratory and 2 health science colleges. There are also 11 sub-city health offices, which are directly accountable to their respective sub-city administration. There are also 52 hospitals in the metropolis of which 6 are owned by Addis Ababa regional health office AARHB, Five by federal government, 3 by NGO’s, 3 by Defense force and police and 35 by the private owners. There are 116 health centres owned by the city administration, and 3 by NGOs at present. There are also more than 760 private clinics at different levels [22]. According to estimates from Ethiopia’s Central Statistical Agency, the Addis Ababa Region’s total population is estimated to be 5.55 million in 2017. Females in the reproductive age group account for 35.5 percent of the overall population [6]. Eight hospitals are operated by the Addis Ababa Health Bureau, seven by the Federal Ministry of Health, one by Addis Ababa University [7]. Those hospitals have different maternity units like family planning, antenatal care, postnatal care and delivery units. There are about 650 mothers delivered in each public hospital in average per month.
Study Design and period
• Institutional based cross-sectional study design was conducted from June 11 to August 30, 2024
Source populations
• All postnatal mothers who was giving birth in Addis Ababa public hospitals
Study population
• All postnatal mothers in selected public hospitals, in Addis Ababa
Study unit
• Each Selected individual postnatal mother in selected public hospitals, in Addis Ababa
Inclusion and Exclusion Criteria
Inclusion criteria
• All mothers who were give birth in the selected study public hospitals were included.
Exclusion criteria
• Post-natal mothers “who was mentally or critically ill during the study period will not be included in the study.
Sample Size and Sampling Technique
The sample size was calculated by using single population formula where p-value was taken from research done in Yeka sub city among mothers’ satisfaction with delivery care services uptake was 63% [45], 95% level of confidence, and 5 % marginal error [8]. Therefore, the required sample size of the study was determined by single population proportion formula as the following.
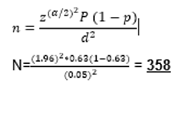 Where, P= 63 %
Where, P= 63 %
Z=level of confidence at 95% certainty (1.96) d= 5% marginal error
Therefore adding 10% of non-response rate it was 394
And the final sample size was taken as 394
|
Variables |
Assumption Sample size |
Sample size |
References |
|
Facility cleanliness |
Margin of error = 5℅, P = 77.9℅, CI=95% |
304 |
14 |
|
Pain management |
Margin of error = 4℅, P = 41℅, CI=95% |
354 |
20 |
|
Privacy in the ward |
Margin of error = 5℅, P = 87.9℅, CI=95% |
255 |
10 |
Table 1: Sample size calculation for specific objectives.
Sampling techniques
Since there are about 12 public hospitals in Addis Ababa, a simple random sampling method was employed to select 30% of the hospitals. There are about 45 mothers in Ras desta Memorial Hospital (RDMH), about 40 mothers in Tirunesh Beijing General Hospital (TBGH), about 50 mothers in Zewditu Memorial Hospital (ZMH), and about 45 mothers were visiting the postnatal ward in Abebech Gobena Maternal and Child Health Hospital (AGMCH) daily. Then the total sample size was proportionally allocated to each selected hospital, and then each individual was selected systematically with every K value in each hospital (k for ZMH = 15, RDMH = 16, TBGH = 15, and AGMCH = 15).
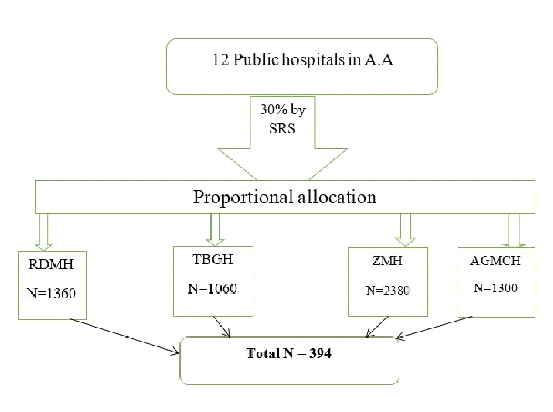
Figure 2. Allocation of the sample of maternal satisfaction in AA public hospitals
Variables of the study
Dependent variable
• Maternal satisfaction on delivery service.
Independent /Explanatory Variable
Structural factors: Availability of infrastructure, Cleanliness of Health facility, Availability of medicines, supplies and services.
Institution related factors
• Cleanliness of health facility
• waiting for time to be seen by a health care provider,
• sex of service providers
Obstetrics related factors
• Neonatal outcome, gravidity, parity
• Time of admission, ANC follow up
• Cost of services
Socio demographic characteristics
• Age
• Marital Status
• Education Level
• Income, occupation
Operational definition
Maternal satisfaction: mothers who scored all satisfaction questionaries’ mean and above was considered as satisfied‖ and those who score below the mean value was considered as unsatisfied [42].
Maternal satisfaction: State of mothers’ expression with delivery care service. It was measured by computing the responses of 32 satisfaction assessing questions categorized into health facility-related (16 questions) and healthcare provider related (16 questions). Each question was rated in a 5-point Likert scale response (i.e., 1 very dissatisfied, 2 dissatisfied, 3 neutral, 4 satisfied, and 5 very satisfied). Then, it was dichotomized as satisfied (if scored above the mean) and not satisfied (if scored below the mean) [20].
The overall mother’s satisfaction was expressed as a state of being satisfied with health care service uptake in the dimension of quality-of-care service (process, outcome, and physical environment).
Satisfied: was measured when mothers scored 75% and above from the items of mother’s satisfaction questionnaire was categorized under “satisfied” [45].
Unsatisfied: was classified when mothers scored below 75% from the items of mother’s satisfaction questionnaire, was categorized under “unsatisfied.” [43].
Data collection tool
Data was collected using a structured questionnaire adapted from different literatures and adapting to the local context. It has also three parts, the first containing Socio demographic characteristics of delivering mothers. The second part was obstetric history of delivering mothers. The third parts contained respondents ‘satisfaction on health facility process, structure and outcome. It was presented using a 5- scale Likert scale (1- very dissatisfied, 2-dissatisfied, 3-neutral, 4-satisfied, and 5-very satisfied). The questioner/tool was primarily developed in English and then translated to the local language (Amharic) and was checked its consistency. And back translated into English again.
Data collection procedure and measurement
Structured questionnaires were used to collect the data after One day training for 10 BSc midwife midwives given. Data collectors were selected from other than the study health centers. To respect the mothers ‘confidentiality to their response, the interview was conducted individually. The selected supervisors were trained on the objective; benefit of the study, individual ‘s right, informed consent and techniques of the interview was told to them. And data was collected from mothers by exit interview in the selected hospital at the time of discharge from the postnatal unit.
Data quality assurance
To assure the data quality high emphasis was given in designing data collection instrument especially socio-demographic and mothers ‘satisfaction parts. Before starting the actual survey, the questionnaire was pre-tested at sent peter hospital in 5% of the study participants. The supervisors conducted supervision and the collected data was checked for completeness on the day of data collection to ensure accuracy of the data during the data collection. The collected data was reviewed and checked for completeness before data entry; the incomplete data was discarded. Data entry format template was produced and programmed.
Data Analysis and management procedures
Data was checked for completeness, coded and entered to Epi-info version 7. Then exported to SPSS (Statistical Package for Social Science) version 26 for analysis. Descriptive statistics was computed and overall level of maternal satisfaction was determined by dividing highest satisfaction Likert scale (five) equally
To identify the association of different independent variables with the outcome variable, cross tabulations and bivariate logistic analysis was carried out. In descriptive statistics tables, graphs mean and frequency was used to present the information. To test Model fitness, Hosmer –Lem show in multivariate logistic analysis was used. Bivariable analysis was analyzed and those p value less than 0.2 was candidate for multivariable analysis and then after those variables whose p value less than 0.05 in multivariate logistic analysis was considered as significance.
Ethical consideration
Ethical clearance was obtained from Ethical review committee of Addis Ababa regional Health Bureau. Then the selected mothers were informed about the purpose of the study, the importance of their participation and their right to withdraw at any time. Data was collected after getting informed consent from mothers. To keep confidentiality, information was given for respondents appropriately and names of respondents were not registered.
Dissemination and utilization of result
Results of the study was to Ayer Tena Health College departments of public health, Addis Ababa health bureau and finally was submitted to Addis Ababa Public health and emergency management directorate.
Result
Socio-demographic status of the study participants
Out of 394 study participants 390 respondents participated in this study making a response rate of 98.99%. About 37.7% of the respondents were aged from 24-29. The mean age of the study subjects were 27.77years (+5.09 SD). The minimum age of the study participants was 19 years and the maximum age was 38 years old. Most participants of the study 363(93.1%) were married. About 285(73.1%) of the study participants live in urban area. (Table 2).
| Variables | Variable | Frequency | |
| Age | ≤ 24 | 117 | 30 |
| 25 – 29 | 147 | 37.7 | |
| 30 – 34 | 71 | 18.2 | |
| ≥35 years | 55 | 14.1 | |
| Marital status | Married | 363 | 93.1 |
| Unmarried | 14 | 3.6 | |
| Widowed | 13 | 3.4 | |
| Educational states | no formal education | 101 | 25.9 |
| primary education | 154 | 39.5 | |
| secondary education | 70 | 17.9 | |
| collage and above | 65 | 16.7 | |
| Occupation | house wife | 199 | 51 |
| Employee | 130 | 33.3 | |
| private employee | 45 | 11.5 | |
| daily labourer | 16 | 4.1 | |
| Income level | < 5000 Ethiopian Birr | 177 | 45.4 |
| ≥5000 Ethiopian Birr | 213 | 54.6 | |
Table 2: Socio-demographic status of post-partum women at public hospital in Addis Ababa Ethiopia 2024.
Obstetrics and Reproductive History of Respondents
Concerning the parity of women, more than half (54.9%) of participants were multipara and nearly all (95.4%) participants pregnancy were wanted. About 377(96.7%) of the participants had normal progress of labour. And those 43(11.00%) of participants labour were started by induction. About 247 participants labour was started spontaneously, and also 372(95.4%) of the pregnancies was wanted while the rest was unwanted. (Table 3).
| Variables (n = 390) | Category | Frequency | Percent |
| Parity (number of births) | Primipara | 176 | 45.1 |
| Multipara | 214 | 54.9 | |
| Gestational age at delivery | Preterm | 16 | 4.1 |
| Term | 356 | 91.3 | |
| Post-term | 18 | 4.6 | |
| Antenatal care visit | Yes | 390 | 100 |
| Onset of labor | Induction | 43 | 11 |
| Spontaneous | 247 | 89 | |
| Birth outcome | Live birth | 381 | 97.7 |
| Dead | 9 | 2.3 | |
| Mode of delivery | vaginal | 235 | 60.3 |
| Caesarean section | 155 | 39.7 | |
| Duration of labor | <12 h | 178 | 45.6 |
| ⩾12 h | 212 | 54.4 | |
| Fetal presentation in labor | Vertex | 356 | 91.3 |
| Non-vertex | 34 | 8.7 | |
| Labor process | Obstructed | 13 | 3.3 |
| Normal | 377 | 96.7 | |
| What was Maternal outcome? | normal | 368 | 94.4 |
| with complication | 22 | 5.6 | |
| Was the pregnancy wanted? | Yes | 372 | 95.4 |
| No | 18 | 4.6 |
Table 3: Reproductive and obstetrics History of Respondents of study participants in Addis Ababa Public hospitals 2024 GC
Health outcome related factors
Among those delivered neonates about 130(40.6%) of participants were. Among those participants 304(95%) were gave birth without complication. Regarding their birth weight about 225(70.3%) mothers gave from 2.5 – 4kg babies. And 316(98.8%) of births were live (Table 4).
| Variables (n = 390) | Category | Frequency | Percent |
| Sex of the neonate | Male | 130 | 40.6 |
| Female | 190 | 59.4 | |
| Birth weight | <2.49 kg | 58 | 18.1 |
| 2.5–4 kg | 225 | 70.3 | |
| >4 kg | 37 | 11.6 | |
| Maternal outcome | Safe | 304 | 95 |
| With complication | 16 | 5 | |
| Fetal outcome | Live birth | 316 | 98.8 |
| Stillbirth | 2 | 0.6 | |
| Neonatal death | 2 | 0.6 |
Table 4: Health outcome related factors of the study participants
Maternal satisfaction with delivery service
Regarding maternal satisfaction with the delivery service, 221 (56.7%) with C.I 51.5 - 60.8 of mothers were satisfied, whereas 169 (43.3%) of mothers were not satisfied with the delivery service (Figure 3).
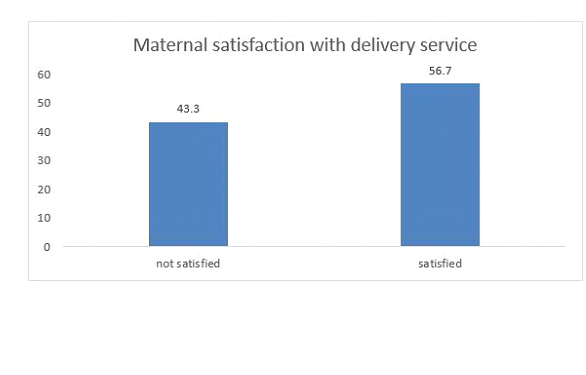
Figure 3: Maternal satisfaction with delivery service of post partum mothers giving birth in AA Public hospital
Factors associated with maternal satisfaction with delivery services
In bivariable logistic regression analysis, residence, parity, ANC follow-up, the onset of labor, duration of labor and sex of the newborn were associated with maternal satisfaction on delivery services
In multivariable analysis, those predictors which showed statistical significance in bivariate analysis and p value less than 0.2 were used to run multivariate analysis. Those participants who delivered without complication were about 7 more satisfied as compared to those participants who delivered with complication AOR =7.177 ( CI: 4.761- 9.698), those participants who had 4 ANC visits and above were about 3.6 times more satisfied than those participants who had under 4 times ANC visits AOR = 3.683(CI: 1.057-10.835), participants who get an income of 5000 and above were about 2 times more satisfied as compared to their counter parts AOR = 2.102(CI:1.025-3.26) (Table 5).
| Variable | Maternal satisfaction | 95% CI | P-value | |||
| YES | NO | COR | AOR | |||
| Mode of delivery | Vaginal | 114 | 121 | 1.713 ( ) | 1.455(0.736-2.875) | |
| CS | 55 | 100 | 1 | 1 | ||
| Maternal outcome | Normal | 162 | 206 | 1.685(1.196-9.888) * | 7.177 (4.761-9.698) ** | 0.003 |
| With complication | 7 | 15 | 1 | 1 | ||
| Age | 20-24 | 52 | 65 | 1.444(0.376-5.551) | 3.477(0.708-17.059) | |
| 25 – 29 | 63 | 84 | 1.303(1.037-1.545) | 2.303(1.327-7.673) | ||
| 30 – 34 | 30 | 41 | 1.444(0.376-5.551) | 3.477(0.708-17.059) | ||
| 35 and above | 24 | 31 | 1 | 1 | ||
| Number of ANC visits | ≥4 | 155 | 182 | 2.226(1.093 -5.543) | 3.683(1.057-10.835) | 0.037 |
| <4 | 14 | 36 | 1 | 1 | ||
| Average monthly income | ≥5000birr | 81 | 96 | 1.199(1.002 -5.328) | 2.102(1.025-3.26) | 0.001 |
| <5000birr | 88 | 125 | 1 | 1 | ||
| Mothers occupation | house wife | 92 | 107 | 1.33(0.68-2.59) | 1.09(0.53-2.27) | 0.042 |
| employee | 50 | 80 | 1.67(1.09-2.57) | 2.20(1.21-4.04) | ||
| private employee | 18 | 27 | 1.33(0.68-2.59) | 1.09(0.53-2.27) | ||
| daily laborer | 9 | 7 | 1 | 1 | ||
Table 5: bivariable and multivariable analysis of maternal satisfaction among laboring mothers in Addis Ababa Public hospitals 2024.
Discussion
This study focused on maternal satisfaction with delivery service and associated factor among post partum women at public hospital Addis Ababa Ethiopia 2024. The overall maternal satisfaction with the delivery service was 221 (56.7%) with (C.I of 51.5 - 60.8). The finding of this study was lower than the studies conducted in Felege Hiwot hospital in Amhara regional state (74.9%) [12], Somalia region (76.6%) [16], Wolaita zone in selected public health facilities (82.9%) [15] and Hawassa public health hospitals (87.7%) [22]. These differences might be due to the study design period, and the difference in place. This difference might be unlike other health facilities there were a high number of client flow in referral and specialized and teaching hospitals. The other probable reason may be the set-up of higher medical institutions not be convenient for mothers due to the complexity of many available services and their costs.
Those participants who delivered without complication were more satisfied as compared to those participants who delivered with complication. According to the study done in Amhara region those mothers who delivered with complication were more decreased in satisfaction [15], according to the study done in St. Paul hospital those mothers who delivered with complication have decreased in satisfaction as compared to their counter parts [17]. The possible reason for this may be due to those who had complication may have pain or some discomfort and may affect their satisfaction. And also, those who delivered with different complication may suffering with pain and may not feeling good. On the other hand, those participants who had 4 ANC visits and above were about 3.6 times more satisfied than those participants who had under 4 times ANC visits. The study done in Addis Ababa health centers those participants who had ANC follow up were about 5 times more satisfied with delivery service [23]. Which may be due to this study is done in Hospitals and there may be high number of ANC mothers and may not have long time to communicate mothers with health care providers. The other possible reason for this may be due to that those participants who had ANC follow up may be more familiar to the service and the staffs of the health institution. And the fact that the advantages of ANC visit to make the mothers well know the area of the service. And some services offered to routine ANC care may more satisfied the mothers. In addition to this those participants who get an income of 5000 and above were about 2 times more satisfied as compared to their counter parts. The possible reason for this may be due to the fact that those participants who get more money may get their need.
However, some variables did not show significance in this study that were associated in other studies. For instance, duration of labor, waiting time, health condition of the fetus, mode of delivery, educational status, occupational status [13], and age [16] were significant in other studies but not in this study. This might be due to variations in the study year, sociocultural differences, sociodemographic differences, variations in the way category of variables, and the countries’ strategies in creating awareness for institutional delivery from time to time.
Limitation
The cross-sectional nature of the study that does not allow for establishing a causal relationship between the different independent variables and the outcome variable could be the potential limitation. In addition, the study might be prone to potential response and social desirability bias as delivery and labor are culturally secret and sensitive issues.
Conclusion and Recommendation
Conclusion
The study examined maternal satisfaction with delivery service and associated factors among post-partum women at Addis Ababa Ethiopia’s public hospital in 2024. Maternal satisfaction with the delivery service was 221 (56.7%), whereas 169 (43.3%). Factors contributing to this satisfaction include Participants who delivered without complications, those with four or more ANC visits, Participants with an income of 5000 or more were 2 times more satisfied.
Recommendation
For Addis Ababa regional health bureau
• Strengthening ANC follow up is recommended
For health care professionals
• Health education and counseling of those mothers to have close ANC follow up
Acronyms
ANC: Antenatal Care; EHCRIG: Ethiopia Hospital Reform Implementation Guideline; EDHS: Ethiopia Demography Health Survey; FMOH: Federal Ministry of Health; HMIS: Health Management Information System; HSTP: Health Sector Transformation Plan; MDG: Millennium Development Goal; MMR: Maternal Mortality Ratio; MWH: Maternal Waiting Home; PHC: Primary Health Care; SDP: Sustainable Development Plan; SPSS: Statistical Package for Social Science; UNFPA: United Nations Population Fund; UNICEF: United Nations Children’s Fund; WHO: World Health Organization.
References