Esther Igboerika1*, Mariea Snell Catherine2
1Fresno Pacific University, 1717 S Chestnut Ave, Fresno, CA 93702, USA
2McAuley School of Nursing, Maryville University, St. Louis, MO, USA
Received: 09 March 2025; Accepted: 24 March 2025; Published: 31 March 2025
Citation: Esther, Igboerika, Catherine M.S. “School-Based Asthma Education Program.” J Healthc Adv Nur (2025): 124 DOI: 10.59462/JHAN.3.1.124
Copyright: © 2025 Igboerika E. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Objective: To compare asthma quality of life among students after an asthma education intervention.
Background: Asthma affects the quality of life of school-age children. Children spend the majority of their time in school. School-based asthma education benefits students, parents, and the school district. Successful school-based asthma education requires care coordination and a team approach. School nurses are well-positioned to provide asthma education.
Methods: A quantitative descriptive study using pretest/posttest design. The Pediatric Asthma Quality of Life Questionnaire (PAQLQ) was utilized. A convenience sample of 19 students in grades 6-8 and ages 11 - 14 completed the KicKin’ asthma education intervention and the PAQLQ. The KicKin’ asthma education was provided once a week for four sessions. The PAQLQ was completed pre and post the KicKin’ asthma education intervention.
Results: Significantly higher PAQLQ scores were seen in each of the PAQLQ domains after the Kickin’ asthma intervention. For activity limitations T=75, z= -2.810 p <. 005, symptoms T=55, z= -2.970 p <. 003, and emotional functions T=79, z= -2.517 p <. 012 respectively.
Conclusion: The KicKin’ asthma education intervention effectively improved the quality of life of middle school students diagnosed with asthma. Asthma education intervention requires care coordination, and school nurses play an essential role in school-based asthma education interventions. Future research can look at resources available to sustain school-based asthma education programs.
The critical element in executing a school-based asthma education intervention is to teach students with asthma how to manage their symptoms, avoid triggers and accurately use their medications properly. Asthma education can be provided to students in the school setting by the nurses. Students spend most of their day in the school, optimizing the school nurse’s ability to implement a comprehensive asthma education program within schools. School nurses are in an ideal position to implement and sustain asthma education. The school nurses act as case managers and are often the healthcare provider that a student regularly sees for acute and chronic illness management. A nurse-led asthma management program is beneficial in the school, and the goal is to provide students with access to asthma care, support them in building self-management skills, and improve their school attendance. [1] reported that the school nurses’ asthma management program decreased school absenteeism and improved inhaler technique. These researchers stated that school nurses’ support could help pediatricians achieve the self-management education element of the National Asthma Education and Prevention Program Expert Panel Report-3 asthma guidelines recommended by the National Institute of Health.
School-based asthma programs can reduce racial disparities in care among children with asthma. [2] reported that asthma prevalence is higher among children living in lower-income and urban communities than children living in higher-income, non-urban areas. Also, schools serving children from low-income communities have higher needs and fewer resources than schools in higher-income communities. The challenges in asthma disparities include coordination of care, a lack of asthma education, and poor medication adherence. These authors suggested that school nurses can serve as navigators to facilitate care coordination and increase parent and student asthma education.
Asthma education programs demonstrate significance for improving symptoms, reducing hospitalizations, and increasing school attendance. The goal of asthma education programs is to help students recognize symptoms and use their medication appropriately. [3] examined asthma education among elementary school students and found a reduction in asthma severity, emergency department (ED), and office visits. [4] reported increased asthma knowledge and symptom management in an asthma program for middle school students. The overall health-related outcomes of asthma education are to improve quality of life, reduce the cost of hospital and emergency room visits, decrease environmental triggers, and enhance physical activity among students with asthma. The non-health outcomes include improving productivity among students and their parents, [4].
This project focuses on a school-based asthma education program. Several research evidences support the implementation of school-based asthma education programs to improve asthma management skills and health outcomes. The literature addressed the school nurse’s role in asthma education, asthma quality of care coordination, elements of school-based asthma education, and asthma education outcomes.
School nurses are in the best position to provide asthma education for children because students spend a significant portion of their day in school. [1, 5, 6] described the importance of asthma programs led by school nurses and the school nurses’ role in improving asthma control among students. The school nurses can facilitate care coordination among HCP and parents and provide information about the student’s asthma control. Through their assessments of students with asthma, the school nurse can provide information about the frequency of daytime symptoms, need for a rescue inhaler, need for follow-up doctor’s visit, physical activity limitations, and frequency of school absenteeism. [5] In the studies by [3, 4, 7, 8, 9] school nurses acted as liaisons. The school nurses played a crucial role in determining inclusion criteria for students’ participation in the studies through their assessments and facilitated communication. These studies also support the value of school nurses in implementing asthma education programs.
A successful school-based asthma program involves the engagement of the HCP, school nurses, parents, and students. Active parental engagement has been a challenge in school-based asthma interventions. Strategies to encourage parents’ involvement and efforts to obtain information about students’ asthma conditions and management from parents are crucial [4, 9]. School nurses are in an optimal position to facilitate care coordination between parents and HCP. The school nurses are familiar with the students and their parents; they have also built a good rapport with them and their families. Also, the school nurses understand the best way to contact parents. Care coordination and collaboration with school nurses could result in the successful implementation of an asthma education program. In the study by [10] the school nurses were not actively engaged, and the research staff was unable to establish communications with parents. As a result, parents’ participation was limited, and only one parent participated in the asthma education session. The study by [1, 3, 5, 6, 11] supported case management and care coordination between HCP, parents, and school nurses. In the study by [6], the school nurses were involved in supervising the asthma program and communicating with HCP and parents. [5] used asthma intake forms to obtain information from parents about the child’s asthma history, such as asthma triggers, prescribed medications, activity performance, HCP contacts, access to medical care, and medication. In contrast, [3] used a health questionnaire and asthma home management survey to enhance parents’ communications.
The study by [5] used an HCP standardized form to communicate information about the student’s asthma control level. It included information such as the need for a home action plan, rescue inhaler treatment in the school, and school absenteeism to the student’s providers. The asthma referral checklist was used by the school nurses as a communication tool with the student’s HCP [1]. The asthma control tests, and asthma action plans were used to communicate between a school, parents, and health care providers [7]. [11] used Primary Care Provider (PCP) Prompt to convey asthma management information and concerns to the student’s providers. Also, Perry et al. encouraged parental involvement by conducting telemedicine asthma education sessions for parents/caregivers on weekdays, weekends, and nights. Other strategies used by these authors to engage parents’ participation are mailing educational materials and providing educational sessions via telephone, providing mobile minutes to parents, and providing transportation vouchers for parents to attend telemedicine sessions.
The National Asthma Education and Prevention Program Expert Panel Report 3 (NAEPP EPR-3) asthma guidelines recommendation on asthma self-management education elements includes inhaler technique, asthma control test, and asthma medication review. The national standard for asthma self-management education includes improving asthma knowledge, symptom monitoring, asthma control, medication adherence, and an individualized asthma action plan [12]. Asthma education elements and curriculum used by most authors in the literature review included asthma triggers, medications adherence, accurate inhaler technique, and communication with HCP [3, 4, 5, 8, 9, 10, 11]. Some of the studies in the literature concentrated on inhaler techniques [1, 6]. [7] mentioned that the students were provided with asthma education but did not indicate the elements or the education curriculum utilized.
School-based asthma education programs are designed to meet the needs of the students and their parents. In the literature review, asthma education was primarily provided to the students [1, 4, 6, 7, 8]. Few of the authors included parents in the asthma program or provided parents with program content handouts [3, 5, 9]. [10, 11] used a different approach in their asthma program. In contrast, [11] provided asthma education to students, parents, and school nurses through telemedicine, [10] provided asthma education to students, parents, and teachers.
Strategies to enhance students’ engagement in asthma education are crucial. In the study by [1, 3, 9] students’ interest and attention were retained using game-like activities, interactive group sessions, and one-on-one coaching. The teaching style used by [8] was interactive; the researchers used videos, posters, comic books, stickers, and a trading card program.
Asthma education programs in school settings have positive outcomes. Several studies have shown that school-based asthma program improves asthma knowledge, symptom control, and self-management skills [1, 3-11]. [8] provided asthma education among elementary students. The researchers found a significant increase in asthma knowledge among the students’ pretest and post-test. The research by [5] demonstrated asthma improvement and increased inhaler technique among students with home asthma action plans, school asthma care plans, and rescue inhalers at school. [1, 5] observed a decrease in school absenteeism and asthma-related emergency department visits among elementary school students that participated in a school nurse-led asthma program. Also, asthma education programs led to improved asthma symptom control and improved self-efficacy [4, 9]. In the study by [7] students’ asthma education and the use of standing orders for albuterol reduced asthma-related emergency medical service calls. Although the studies by [3, 10] were not statistically significant, these authors noted improvement in participants’ self-management behaviors.
The DNP project was implemented in an elementary school district in the Western region of the United States, serving low-income and medically underserved communities with an increased rate of childhood asthma. The participants included a convenience sample of students diagnosed with asthma in 6th, 7th, and 8th grades. Students’ health records from the school district were used for data collection. Students with a diagnosis of asthma in their school health records and students with asthma medication orders were recruited by the various school nurses at the school sites. The participants were engaged in either online or in-person asthma education intervention. The participants completed the Kickin’ asthma education [13]. The Kickin’ asthma education consisted of four 45-minute sessions, and the curriculum includes:
A quantitative, exploratory design through a pre/posttest was utilized to measure asthma quality of life. This project was reviewed by the Institutional Review Boards at Maryville University (see Appendix E). Parental consent and students’ assent were obtained (see Appendices D, E, and F).
Before this quality improvement project, no consistent asthma education was provided to students to improve asthma management. Students are provided with asthma education by their health care provider or parents. The school nurses provide asthma education, mostly inhaler techniques, to students who have authorization from a medical provider to self-administer their inhalers. This quality improvement program was implemented to improve asthma quality of life among students and increase their asthma self-management skills. School-based asthma education programs improve asthma knowledge, symptom control, and self-management skills [1, 2, 14].
The anticipated number of participants was 30 students. The age ranges of the students are between the ages 11-14 years old, including male and female and all ethnic/racial groups.
The inclusion criteria for participating in the project include:
The exclusion criteria for participants include:
A step-by-step outline of the project’s protocol is as follows:
The Pediatric Asthma Quality of Life Questionnaire (PAQLQ) was used before and after the asthma education intervention to assess the impact of asthma on participants. The PAQLQ is a validated survey that measures the physical, emotional, occupational, and social problems of children 7-17 years with asthma. The PAQLQ also has strong reliability; it contains 23 questions subdivided into three domains: asthma symptoms, activity limitations, and emotional functions. The PAQLQ is a seven-point response scale that ranges from 7 (no impairment), 4 (moderate impairment), and 1 (severe impairment). The PAQLQ score is obtained through the mean of all the answers to the questions.
The KicKin’ asthma education intervention was implemented after obtaining institutional review board (IRB) approval from the university, permission from the school district, and parental consent. This quality improvement project was considered exempt from human studies regulation by the IRB. A permission letter was obtained from the American Lung Association to implement the KicKin’ asthma education program. Also, Professor Juniper, the author of the questionnaire, granted permission to use the PAQLA. The school nurses of the selected sites supported the recruitment phase and the asthma education class schedule. All recruited participants were evaluated for inclusion criteria, and those with no exclusion conditions were assigned a number. During the education intervention, participants were separated by grades (6th, 7th, and 8th) due to their different class schedules. The following data were entered in the Excel sheet
Ethical considerations included the protection of participants’ rights and data collection sheets. The risk is a breach of confidentiality, and coercion was minimized. All participant identifiers were removed, data collection sheets were locked in a file cabinet, and electronic data were stored in a password-protected computer. Project participation was voluntary. Participants were permitted to withdraw from the project at any point. Participants had access to school health care services regardless of whether they participated or withdrew from the project.
The KicKin’ asthma education was provided in person to participants that met the inclusion criteria. The instructor’s manual, student’s workbooks, scenario activities/games, demonstration equipment such as a peak flow meter, spacer, inhaler, pictures, and videos were utilized during the asthma class. The KicKin’ asthma education was implemented every Tuesday during the physical education class period in the school library. Four 45-minute sessions were scheduled for four weeks. During the first session, the participants completed the pre-intervention PAQLA. They also received the KicKin’ asthma workbook. The workbooks were kept in the library after each session, except the fourth session. At the end of the fourth session, the participants took their workbooks home, and they were encouraged to refer to the workbook as needed and share their learning experiences with their parents and guardians. The participants also received an aero chamber for their inhalers at the end of the fourth session.
The PAQLA was used before and after asthma education intervention. This questionnaire measures children with asthma’s physical, emotional, and social problems. It can be used for children between the ages of 7- 17 years. The self-administered version of the questionnaire was utilized for this project.
The questionnaire consists of 23 items that are divided into three domains: symptoms (10 items), emotional functions (8 items), and activity limitations (5 items). The response options to the 23 items are on a seven-point scale that ranges from 7 (no impairment), 4 (moderate impairment), and 1 (severe impairment). The overall score of the PAQLQ is calculated by using a mean of all the J Healthc Adv Nur 2025; Vol. 3(1) Page - 6 Igboerika E answers. The wording of each item in the questionnaire are words children use to describe their asthma problems.
Children can understand the questions and answer based on their asthma problems. The estimated reliability score within the subject standard deviation is 0.17, with an intraclass correlation coefficient (ICC) of 0.95 overall. The overall ICC score demonstrates the instrument’s strength in discriminating between subjects with different impairment levels. The ICC score is consistent through each PAQLQ domain and the different age groups; this means that children aged 7-17 can competently complete the PAQLQ. The PAQLQ has good cross-sectional and longitudinal validity; it can be used as an evaluative and discriminative instrument. It shows aspects of asthma that are most important to the patient and provides information on clinical outcomes.
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS 26). The data analysis was conducted with the assistance of Dr. Pahls, Maryville University’s statistician. There were missing data. Participants that did not complete the asthma class and the post-tests were excluded. This quantitative research design compares the differences between the pretest and post-test scores of the PAQLQ using the Wilcoxon Signed Ranks Test.
A total of 23 participants in grades 6th, 7th, and 8th graders were recruited to participate in the KicKin’ asthma education intervention, with 19 participants (82.6%) completing the asthma class and the pre and post-tests. The participants were between the ages of 11 and 14 years. Twelve participants (52.2%) were in 6th grade, five (21.7%) were in 7th grade, and two (8.7%) were in 8th grade (Table 1).
The KicKin’ asthma education class started in April after Spring Break and continued through the end of May. The PAQLQ pretest was obtained during the first session of the KicKin’ asthma intervention, and the PAQLQ post-test was completed at the end of May 2022. Four participants were absent from the fourth-class session and could not complete the post-PAQLQ. Participants’ absences were related to covid symptoms and positive cases. A sample size of 35 was needed to provide an effect of 0.5, with a significance of 0.05 and a power of 0.8. The sample size included in this study did not meet the minimum amount needed for the study. A Wilcoxon’s test was calculated to compare PAQLQ scores before and after asthma education class. A significant difference was found between pre and post-test for the three domains (symptoms, activities limitations, and emotional functions). For activity limitations T=75, z= -2.810 p <. 005, symptoms T=55, z= -2.970 p <. 003, and emotional functions T=79, z= -2.517 p <. 012 respectively (Table 2).
Table 1. Demographics
| Group 1 | Group 2 | Group 3 | |
|---|---|---|---|
| Age | 11-12 | 12-13 | 13-14 |
| Grade | 6th | 7th | 8th |
| No of participants | 12 | 5 | 2 |
Table 2. Test Statisticsa
| Activity limitations post-test – Activity limitations pre-test | Symptoms post-test- Symptoms pre-test | Emotional functions Post-test- emotional Functions pre-test | |
|---|---|---|---|
| Z | −2.810b | −2.970b | −2.517b |
| Asymp. Sig. (2-tailed) | 0.005 | 0.003 | 0.012 |
a. Wilcoxon Signed Ranks Test
b. Based on negative ranks.
A bar chart was used to compare the difference between the pre-invention and post-intervention PAQLQ scores in the activity limitation domain (Figure 1). The degree of asthma impairment was grouped into severe impairment (1-3), moderate impairment (4-5), and no impairment (6-7). Before the asthma education intervention, four participants (21.1%) had a severe impairment, six participants (31.6%) had mild impairment, and nine participants (47.4%) had no impairment. After the intervention, two participants (10.5%) had an impairment, four participants (21.1%) had moderate impairment, and 13 participants (68.4%) had no impairment.
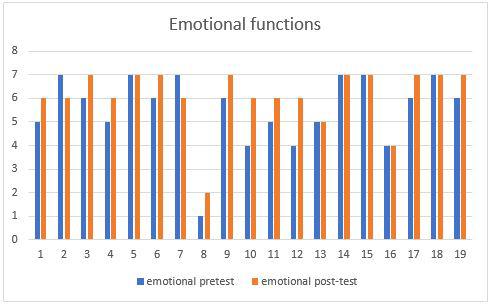
Figure 1. PAQLA Domain: Activity Limitations
Based on the data collected, there was an improvement in symptoms (Figure 2). Before the asthma education intervention, five participants (26.3%) had a severe impairment, six participants (31.6%) had mild impairment, and eight participants (42.1%) had no impairment. After the intervention, three participants (15.8%) had a severe impairment, four participants (21.1%) had a moderate impairment, and twelve participants (63.1%) had no impairment.
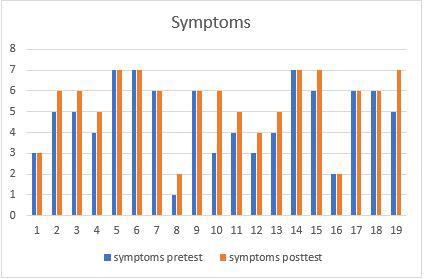
Figure 2. PAQLA Domain: Symptoms
Before the asthma education intervention, one participant (5.3%) had a severe impairment, seven participants (36.8%) had mild impairment, and eleven participants (57.9%) had no impairment. After the intervention, one participant (10.5%) had a severe impairment, two participants (10.5%) had a moderate impairment, and 16 participants (84.2%) had no impairment (Figure 3).
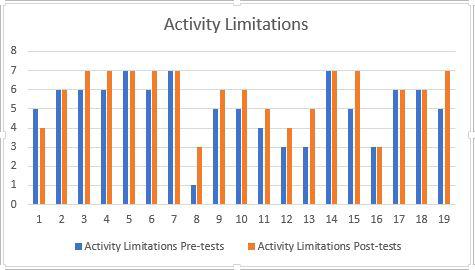
Figure 3. PAQLA Domain: Emotional Functions
This project was conducted in a rural school district and a region where asthma impacts the life of school-aged children. Before this quality improvement program, students with asthma learn about their health conditions from their parents or health care providers. The school nurses also teach students inhaler techniques occasionally. There was no school-based asthma education program. Also, students struggled to manage their asthma at home and school. This quality improvement program was implemented to improve asthma quality of life among students and increase their asthma self-management skills. Also, implementing an asthma education program led by school nurses may increase program sustainability. School-based asthma education programs improve asthma knowledge, symptom control, and self-management skills [1, 2, 14].
The results revealed statistically significant differences in post-PAQLQ scores for activity limitations, symptoms, and emotional functions. There was an increase in the number of participants with no asthma impairment. The objective was to develop a nurse-led school-based asthma program and improve asthmatic children’s quality of life was met.
The Kickin’ Asthma education intervention addressed asthma quality of life concerns among school-aged children. As teens grow, they become independent and can understand and manage their asthma conditions. The measurements of activity limitations, symptoms, and emotional functions in the PAQLQ are used to determine the degree of asthma impairments among the participants. The results showed a decreased severity of asthma impairment. No asthma impairment may indicate that the student’s asthma was well controlled. Well-controlled asthma includes understanding asthma symptoms/warning signs, staying away from triggers that set off their asthma, and using asthma medication correctly/consistently as prescribed by the health care providers. The purpose of the KicKin’ asthma program was to teach students self-management skills and reduce their asthma symptoms and illness, hence improving their health outcomes.
This project was designed to improve the quality of life of students with asthma diagnoses. The asthma education intervention utilized was the Kickin’ asthma program from the American Lung Association. The primary goal of the KicKin’ asthma education is to improve self-management skills among children with asthma. A quantitative, exploratory design through a pre/post-test was utilized to measure asthma quality of life. The Wilcoxon Signed-Rank test was used to compare PAQLQ scores before and after the asthma education intervention. The results showed significant differences between pre and post-test for the three PAQLQ domains (symptoms, activities limitations, and emotional functions). The degree of asthma severity decreased among participants in both symptoms, activity limitations, and emotional functions. The objective was to develop a nurse-led school-based asthma program and improve asthmatic children’s quality of life, which was met.
The timing of the program implementation was challenging due to several school activities and COVID-19 pandemic, but the program outcomes were met, and the program was valued by students, parents, teachers, and the school administrator. For students to fully benefit from the program outcomes, the KicKin’ asthma education intervention can be implemented at the beginning of the school year. Also, implementing the program at the beginning of the school year may reduce scheduling barriers as the end of the school year is the busiest time due to several school activities and academic testing.
The outcome of this project produced a significant improvement in the asthma quality of life test scores from pretest to posttest intervention. Participants’ engagement in the KicKin’ asthma education intervention resulted in decreased asthma impairment in the symptoms, activity limitations, and emotional function domains of the PAQLQ questionnaire. This project demonstrates that the KicKin’ asthma education can be provided in school to improve the quality of life of young teens and adolescents with asthma. This project also provides evidence that school-based asthma intervention programs are beneficial to students. Several factors such as project timeline, COVID-19 pandemic, asthma education class scheduling, and researcher knowledge of school nursing played a role in the study outcomes. Practice implications and research recommendations will be discussed in the next chapter.
The outcome of this project produced a significant improvement in the asthma quality of life test scores from pretest to posttest intervention. Participants’ engagement in the KicKin’ asthma education intervention resulted in decreased asthma impairment in the symptoms, activity limitations, and emotional function domains of the PAQLQ questionnaire. This project demonstrates that KicKin’ asthma education can be provided in the school to improve the quality of life of young teens and adolescents with asthma. This project also provides evidence that school-based asthma intervention programs benefit students. School-based asthma education interventions described in this project are similar to those found in the literature, such as asthma quality of care coordination [1, 3, 5, 6, 11], school nurse’s role in implementing asthma program [1, 5, 6], elements of School-based asthma education [3-5, 8-11] and asthma program outcomes [1, 3-9, 11].
Care coordination and a collaborative team approach are feasible in implementing an effective asthma program in the school. This study demonstrates that school nurses can provide an asthma education intervention. Collaboration with school administrators, teachers, and parents is essential in implementing an effective school-based program. The study by [3, 4, 9] supported the value of the school nurses in implementing asthma programs.
Regarding the quality of life, the project showed significant improvements in the symptom domain, activity limitations, and emotional functions of the PAQLQ. There was no pre-test and post-test determination in the study by [4]. Although the asthma education contents were similar to this study, [4] included communication with health care providers as a part of their program curriculum. The KicKin’ asthma curriculum provided an emphasis on advocacy and problem-solving skills.
This project has essential strengths. The project was conducted in a region where asthma has a significant negative impact. Also, the collaborative team approach used in this project demonstrated that the asthma education program could be successfully implemented; this approach will facilitate the program’s sustainability in the school environment. The pre and post-test questionnaires were used to evaluate the effectiveness of the education intervention. The PAQLQ and the KicKin’ asthma education addressed behavior and emotional concerns associated with uncontrolled asthma. This study’s education intervention met the national asthma self-management education standards. It addressed essential components of asthma self-management skills such as asthma knowledge, identifying and preventing triggers, symptom monitoring/asthma control, inhaler technique, and medication adherence [12].
There are limitations to this study. The sample size of this study is small. A larger sample size is needed to provide more data on the impact of this program. There were also missing data as some participants could not complete the asthma education sessions and posttest questionnaires due to the implications of the COVID-19 pandemic. Data were only collected from participants who completed the education interventions, pretest, and posttests. Also, the project outcomes were measured only once. This project would benefit from a more-extended follow-up period as it takes time to achieve self-management skills to manage a chronic disease like asthma. There is no control group in this project; it is difficult to determine whether students that are not enrolled in the program would have improved in the symptom domain of the PAQLQ. Students with asthma received education about inhaler techniques and symptom management when the school nurse observed that they were not using their inhalers correctly or having consistent asthma symptoms.
This project characterizes generalizability as the educational intervention used can be provided to asthmatic students in 6th -12th grades. Also, the PAQLQ measures asthma quality of life in children aged 7-17 years. The generalizability of project findings may be limited. Participation was limited to students with parental consent. Also, due to project timing, only two elementary and one middle school participated in the school-based asthma program. These students might not represent all students with asthma in the school district.
The sustainability of this project can be attainable if all the school nurses become facilitators for the KicKin’ asthma education program. The students’ experiences doing the KicKin’ asthma classes were perceived as positive; and the students were able to interact with each other, and all participated in the discussions, games, and scenarios. Positive feedback was received from the school nurses, parents, class teachers, and physical education teachers. The students that participated in the program have shown improvements in medication compliance. The school nurses shared that these students have been coming to use their inhalers before physical activities without reminders. The physical education teacher shared that the students are accepting and willing to participate in physical activities. Some parents shared that they have noticed the independence of the participants in following their asthma action plan at home. The teachers and school administrators suggested program implementation be provided at the beginning of the school year so that students can benefit from the program throughout the school year.
Some barriers identified in this project included a lack of comprehensive resources to implement a sustainable school-based asthma program, parental and staff engagement, and COVID-19 school-related absences. The impact of COVID-19 was a significant barrier as some participants were affected and could not complete the program. Also, participants recruitments were put on hold several times because of the COVID-19 surge in the school. The implementation of the project was during the end of the school year, and the timing was short to recruit more participants for the project. The anticipation was to include five elementary and two middle schools, but only one elementary and one middle school participated in the project.
The facilitators of this project included strong coalition team members, the school site principal, nursing director, the school site nurses, a physical education teacher, a resource teacher from the student success team, a parent club member, and two students from the asthma support group. These groups of individuals worked together to communicate program goals and outcomes. The American Lung Association provided most of the resources needed to implement this program.
The feasibility of this project demonstrated improvement in all domains (symptoms, activity limitations, and emotional functions) of the PAQLQ scores after an asthma education intervention. The participant’s engagement in the KicKin’ asthma education resulted in decreased asthma impairments in their symptoms, activities limitations, and emotional functions.
Evidence indicates the importance of asthma education and quality of life. There is a need for asthma education in the school as the time spent in the outpatient clinic is short. The feasibility of this project demonstrated improvement in all domains of the PAQLQ. Uncontrolled asthma continues to negatively impact students, families, and the school with implications for quality of life, including health and academic outcomes. Since children spend most of their time in school, a comprehensive and effective school-based asthma education is convenient, accessible, and can close the gap of asthma disparities and morbidity.
A school-based asthma management program is cost-effective and can decrease avoidable health care costs. The economic burden associated with childhood asthma in the United States is significant and continues to grow over time. Poorly managed asthma can lead to frequent hospitalization and emergency room visits, increasing health care costs, decreasing school district funding due to absenteeism, and losing productivity from parents. Implementation of a school-based asthma program is cost-efficient. A future effort will be to expand resources for school-based asthma programs.
School-based asthma policies provide students with asthma access to services, support them in building self-management skills, and improve their health outcomes. School nurses serve as case managers and are often the healthcare provider that a student sees regularly. School nurses act as a liaison between health care providers, parents, students, and the school staff. This study demonstrates that school nurses can implement asthma education, and this support from the school nurses can help achieve self-management education of the National Asthma Education and Prevention Program.
School nursing practice support and policies are needed to achieve an effective and sustainable asthma education program. According to the Asthma and Allergy Foundation of America (2019), the recommended policies to improve asthma management and care in schools include a nurse-to-student ratio of 1:750 or better, one full-time nurse per school, and school nurses serving as a case manager for students with chronic conditions such as asthma. Appropriate staffing of school nurses and evidence-based training about asthma management for school nurses is required to implement effective school-based asthma management. This project supports school nurses’ role in asthma management and care coordination.
The quality of care provided to students in the school setting is crucial, and these care qualities influence students’ school attendance and academic performance. The presence of asthma symptoms can result in a lack of sleep, leading to poor attention in the classroom, failure to complete schoolwork, and limitations in physical and social activities. Poorly managed asthma may lead to frequent hospitalizations, emergency department visits, and chronic school absenteeism. Many children with a history of asthma do not practice self-management of asthma effectively. Asthma educational programs are the cornerstone for effective asthma self-management.
This project demonstrates that a school-based asthma education program is a feasible intervention that could improve the quality of life of students with asthma. The KicKin’ asthma education intervention led to a significant improvement in all domains of the PAQLQ. An effective and sustainable school-based asthma education program requires care coordination and team collaboration. This project supports the role of the school nurse in implementing an asthma education program. Future research is needed to examine strategies and resources to support school-based asthma education programs.