Yusuf Coşkun1,Sevil Güler2*
1Nurse Yusuf COŞKUN
2Associate Professor Department of Nursing, Erciyes University Faculty of Health Sciences, Kayseri, Turkey
Received: 11 July 2025; Accepted: 31 July 2025; Published: 04 Aug 2025
Citation:Yusuf, Coşkun, Sevil Güler“The Effect of Shotblocker on Pain Vıolence and Injectıon Satısfactıon in Subcutaneous Injectıon In Adults: A Randomized Controlled Trial.” J Healthc Adv Nur (2025): 126 DOI: 10.59462/JHAN.3.2.126
Copyright: © 2025 Güler S.. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Aim: Nurses are the primarily responsible people in
relieving pain of patients and eliminating their anxiety
during the the Subcutaneous (SC) injections. This study
was conducted to determine the effect of ShotBlocker
on pain level and injection satisfaction in SC injection
administrations.
Methods:A randomized controlled experimental research design was used. The data were collected using
the patient information form, the Visual Analog Scale for
Pain (VAS), the Visual Analog Scale for Patient Satisfaction (VASPS), and Shotblocker.
Results:The injection pain levels of the individuals in
the intervention group were measured by using VAS
pain scale and their pain severities were found to be
lower than those of the control group (p <0.05).
Conclusions: It was determined that the use of shotblocker during SC injection decreased pain levels and
increased injection satisfaction.
Clinical trials registration number: https://clinicaltrials.
gov; NCT05647239.
The critical element in executing a school-based asthma education intervention is to teach students with asthma how to manage their symptoms, avoid triggers and accurately use their medications properly. Asthma education can be provided to students in the school setting by the nurses. Students spend most of their day in the school, optimizing the school nurse’s ability to implement a comprehensive asthma education program within schools. School nurses are in an ideal position to implement and sustain asthma education. The school nurses act as case managers and are often the healthcare provider that a student regularly sees for acute and chronic illness management. A nurse-led asthma management program is beneficial in the school, and the goal is to provide students with access to asthma care, support them in building self-management skills, and improve their school attendance. [1] reported that the school nurses’ asthma management program decreased school absenteeism and improved inhaler technique. These researchers stated that school nurses’ support could help pediatricians achieve the self-management education element of the National Asthma Education and Prevention Program Expert Panel Report-3 asthma guidelines recommended by the National Institute of Health.
School-based asthma programs can reduce racial disparities in care among children with asthma. [2] reported that asthma prevalence is higher among children living in lower-income and urban communities than children living in higher-income, non-urban areas. Also, schools serving children from low-income communities have higher needs and fewer resources than schools in higher-income communities. The challenges in asthma disparities include coordination of care, a lack of asthma education, and poor medication adherence. These authors suggested that school nurses can serve as navigators to facilitate care coordination and increase parent and student asthma education.
Asthma education programs demonstrate significance for improving symptoms, reducing hospitalizations, and increasing school attendance. The goal of asthma education programs is to help students recognize symptoms and use their medication appropriately. [3] examined asthma education among elementary school students and found a reduction in asthma severity, emergency department (ED), and office visits. [4] reported increased asthma knowledge and symptom management in an asthma program for middle school students. The overall health-related outcomes of asthma education are to improve quality of life, reduce the cost of hospital and emergency room visits, decrease environmental triggers, and enhance physical activity among students with asthma. The non-health outcomes include improving productivity among students and their parents, [4].
Keywords:Injection Satisfaction; Pain; Shotblocker; Subcutaneous Injection.
Subcutaneous (SC) injection, one of the parenteral drug administrations, is the process of injecting small amounts of drugs into the loose connective tissue under the dermis layer with the help of special injectors [1,2]. In case of incorrect administration of subcutaneous injections in which drugs with low molecular weights like heparin, insulin, morphine and vaccine are administered, complications such as pain, echymosis or hematoma are frequently seen in the injection site. It is extremely important to considering the personal, developmental characteristics and health status of the individuals and ensure the patient safety in order to minimize this problem [3,4]. Due to high number of pain receptors in the subcutaneous tissue, patients often experience pain [5,6]. The pain that comes with subcutaneous heparin treatment not only causes physical trauma in patients but also leads to a change in their body image. If the patient expresses that he/she has too much pain after SC injection, this is thought to be related to anxiety increase or to the previous events. Therefore, patients may experience reluctance, displeasure, and dissatisfaction during injection practices performed at repeated intervals and doses in particular, as a result of the discomfort they feel after SC injection [7].
Pain experienced during and after the injection deteriorates the comfort of the individuals and may lead them to prejudice against the next injections [4,8]. In addition, it is caused for the person who will do the injection to have difficulties in selecting the site for the following injections. This is because the use of the damaged site in subsequent injections causes the development of pain in the site and negatively affects the absorption of the drug [8-10].
Subcutaneous tissue is very sensitive to large amounts of irritant drugs. Therefore, only a small amount (0.5-1ml) should be administered and should not exceed 2 ml [4,11]. Preventing the problems caused by undesirable effects of parenteral drugs and incorrect injection practices is one of the most important tasks and responsibilities of nurses. In the studies, many applications are recommended to prevent or minimize the complications in SC injections [3]. In a study conducted by Dadaeen et al., to determine the effect of the pressure time applied to the injection site after heparin injection on pain level, pressure was applied to the control group for 10 seconds after heparin injection and to the intervention group for 30 seconds and a significant decrease was determined in the pain level and development of echymosis in the intervention group [12]. Similarly, Yi et al., applied heparin injection to the patients separately for 30 secs and 10 secs in order to determine whether or not SC injection time affects the pain level and they found that echymosis and pain intensity decreased in injection sites of SC injection administered for 30 seconds, time of SC heparin injections affected the complications and it was recommended to administer injection within 30 seconds [13].
In a study conducted to compare abdominal and deltoid regions of patients using subcutaneous heparin in terms of pain level, injections were administered with 24-hour interval so that the first injection was administered to the right deltoid region and the second one was administered to the abdominal region, echymosis and hematoma were assessed at the 48th hour after each injection and the pain level was assessed immediately after the injection, and its duration was assessed during the injection. As a result of the study, mean pain level scores were found to be lower in the abdominal region and the use of abdominal region was recommend for subcutaneous heparin injections14.
In another study systematically investigating the studies on preventing pain associated with subcutaneous heparin injection, the researcher investigated the effectiveness of various applications for the prevention of subcutaneous heparin injection- associated pain, echymosis and hematoma. These applications included injection duration of the drug, waiting time of the drug before removing injector, local cold application to the site before and after injection, pressure and topical applications, selection of injection area, aspiration and airlock techniques. As a result, it is recommended to administer subcutaneous heparin injection in 15-30 seconds, perform local cold application to the injection site for 2 minutes, apply local pressure after injection, prefer abdominal region, and conduct air lock technique applications without aspiration application in order to minimize the local side effects of subcutaneous heparin applications [15].
In the study conducted by Dragoet al., with 85 children, Shotblocker was used to reduce intramuscular injection pain. While no difference was found in the pain assessments of children, a general view appeared on that the pain scores of children decreased according to the assessments of nurses and caregivers [16].
In order to reduce complications associated with SC injection and develop different options, it is necessary to find and implement new non-pharmacological methods. Shotblocker is a plastic tool that can be applied to every age group, is easy to use and inexpensive, can be applied by a single person without requiring any additional material, has blunt and short protrusions with 2 mm thickness providing connection with skin during injection, is applied by holding on skin, and prevents the sensation of pain during injection and its transmission of that pain to the central nervous system by applying temporary blockage to the peripheral nerve ends [17].]The stimulation generated by Shotblocker blocks pain signals, which are slower during the injection, temporarily and decreases pain by closing the gates to the central nervous system [18]. In a quasi-experimental study conducted by Aydın in 2015, the effect of Shotblocker on 50 patients receiving intramuscular diclofenac sodium therapy was evaluated. It was determined that Shotblocker was an effective method in reducing pain associated with IM injection [17].
It is seen that the number of studies conducted to determine the effect of Shotblocker is limited and it is applied only to intramuscular injection technique. New and further studies are needed to support the studies with tried and proven applicability. This study was needed to relieve the pain experienced with SC injection which is a practice performed by nurses, to increase patient satisfaction, to increase the patient’s adaptation to the treatment, and to establish positive patient-nurse communication.
The hypotheses of the study were as follows:
H1: Shotblocker is effective on pain level in subcutaneous injection administrations.
H2: Shotblocker is effective on injection satisfaction in subcutaneous injection administrations.
Study design
The study was conducted in a randomized controlled study design in order to determine the effect of Shotblocker on pain and injection satisfaction in patients who were using DMAH and received subcutaneous injection after arthroplasty surgery in orthopedics training clinic.
Sample
The population of the study was composed of the patients staying in the Orthopedic Clinic in Kayseri Training and Research Hospital due to the diagnosis of arthroplasty. The data of 2016-2017 were taken as a reference in determining the population. The number of patients who underwent arthroplasty surgery in the previous year in the orthopedic training clinic was 402.
In the sample selection of the study, the studies in the literature were taken into account [14,19]. According to statistical consultancy, as a result of the calculation made confidence interval of with 95% and error margin of 0.05, it was considered appropriate to include 50 patients in the intervention group and 50 patients in the control group. By predicting that there may be patient loss, it was decided to include additional 10 patients in both groups and the study was started with a total of 120 patients. The study was completed with a total of 120 patients (60 in the intervention and 60 in the control group) meeting the inclusion criteria between 04.12.2017 and 01.05.2018. (Figure 1) shows a flow diagram of the study.
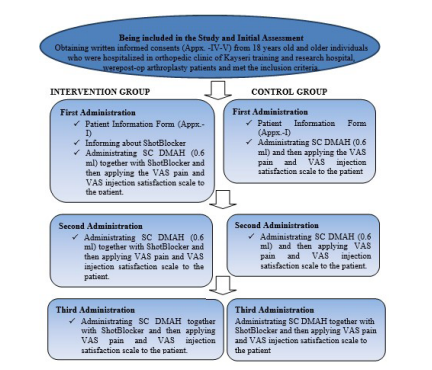
Figure 1.Flow Diagram
Inclusion criteria:Individuals whose treatment plan was Clexane 1x1 0.6 mg subcutaneous, who were over 18 years of age, were conscious, had cognitive competence to answer the questionnaire, had no vision and hearing loss, had no bleeding clotting disorder, had platelet, INR and APTT values within normal limits, had no signs of scar tissue, incision or infection in the injection site, had no allergy history and agreed to participate in the study were included in the study.
Exclusion criteria:The patients, who had amputation in the right/left arm region to be injected, had any scar tissue, incision, lipodystrophy or infection symptom on the injection site in the arm area, received hemodialysis treatment and had dialysis catheter, underwent mastectomy surgery and should not receive any practice/treatment on the arm on the operated side, were excluded from the study.
At the end of the study, in the comparison of the intervention and control groups at 95% confidence interval, the power was found as 0.99 for VAS pain and VAS injection satisfaction and the sample size was decided to be adequate. The selection of the intervention and control groups of the study was determined according to the randomization made in the computer environment. Data collection started on 04.12.2017.
Randomization and intervention
Intervention group:Before starting the application, the researcher informed the patients in the intervention group about the purpose of the study and their verbal and written informed consents were obtained.
The individuals to be included in the intervention and control groups were randomized by a faculty member at the Biostatistics Department of a university in the computer environment. The application was initiated by including the patients meeting the inclusion criteria on 04.12.2017. During the study, no intervention was made on the routine treatments of the patients in the intervention and control groups. Before the application, patient information form of each patient was filled using face-to-face interview technique.
Since the patients included in the study were discharged early (mean hospitalization duration was 3 days), the first, third and fifth SC heparin injection (0.6 ml) administrations were performed by the researcher for three days. The application was made to the arm area due to the fact that Shotblocker was difficult to place in the abdominal area, and the outer side of the arm was preferred for subcutaneous injection administrations in the clinic where the study was conducted. Shotblocker was placed on the injection site determined on the outer side of the upper arm of the patient and the injection was administered by gently pressing the tool with the fingertips during the injection. Shotblocker was removed after removal of the injector. Injections were completed in 20 seconds and the injection site was supported with cotton for 30 seconds. In the first minute after each SC injection application, the patients were asked about the pain level felt during the injection and the injection satisfaction status.
Control group:Verbal and written informed consents of the patients included in the control group were obtained after they were informed by the researcher. Before the application, questions in patient information form were asked to each patient and how to use the VAS pain and injection satisfaction scale was explained. During injection, SC Clexan (0.6 ml) was injected on the site without using Shotblocker. Injections were completed in 20 seconds and the site was supported for 30 seconds. In the first minute after each SC injection administration, the patients were asked about pain level felt during the injection and injection satisfaction status.
In this study, the researcher administered all SC injections by throughout the study by considering the reliability of the study results.
The data of the study were collected using patient information form, VAS Pain (Pain Level Measurement) and Visual Patient Satisfaction Scale. In the study, ShotBlocker was also used to administer subcutaneous injection to the patients.
Patient information form
It was prepared by the researcher by reviewing the related literature and studies [20-23]. The form has 5 questions about some socio-demographic characteristics of the individual (age, gender, marital status, educational status, working status etc.) and 9 questions about the characteristics related to health, disease, and treatment (presence of chronic disease, condition of continuous medication, body mass index, laboratory results, etc.).
Pain Level Measurement -Visual Analog Scale (VAS)
The scale developed by Priceet al., (1983) was used to evaluate the pain level perceived subjectively in many studies and found to be valid and reliable. The scale is composed of a 10-cm vertical or horizontal line starting with “no pain” and ending with “worst pain”. The patient sare asked to indicate the severity of their pain by marking the appropriate point they see appropriate. The distance between the “no pain” starting point and this point is measured and recorded as “cm”. The values range between 0 and 10 and the pain levels of patients are evaluated over 10 points as 0=no pain and 10=worst pain [24].
Visual Patient Satisfaction Scale (VAS)
Visual patient satisfaction scale is composed of a 100-mm horizontal line without numbers. The statement of “I am completely dissatisfied” is present on one end of the line and the statement of “I am completely satisfied” is present on the other end of the line. The patient should identify the satisfaction situation by synthesizing all the components affecting him/her about the medical care given and find the point corresponding to his/her condition on the line [25].
ShotBlocker
ShotBlocker is a small plastic tool that can be used in all age groups in reducing pain due to injection, is nonmedicinal, non-invasive, easy to use, and inexpensive and does not require material preparation (Figure 2). It is used by being held on the skin surface during injection. It has no known side effects [16,17]. ShotBlocker is a patented tool developed to reduce injection pain and anxiety. It was designed for the application of intramuscular and SC injections [25]. ShotBlocker has short, blunt protrusions on one side that provide a connection with the skin and there is an opening in its middle part for easy injection. The pointed surface of the tool is placed on the area to be injected just before the injection. The points on the surface of ShotBlocker do not penetrate into the skin and it is thought be provide stimulation for the Gate Control Theory which is considered to exist regarding pain [23,26].
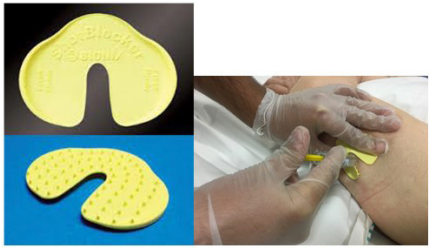
Figure 2.Shotblocker and its application
Statistical analysis
The data were formed and evaluated by using IBM SPSS Statistics 25 software packages. Socio-demographic characteristics of the participants were examined by using Chi-square analysis and independent samples t-test. While the individuals’ disease-related characteristics were examined with chi-square analysis, some laboratory results were examined by using independent samples t-test. The distribution of numerical variables was evaluated by Shapiro-Wilk normality test. VAS pain score and injection satisfaction variables were examined with independent samples t-test within the follow-up groups and when all the follow-up groups were considered, they were examined by using Repeated Analysis of Variance. The homogeneity of the variances was tested by using Levene’s test. In case that there is a difference between groups, Tamhane multiple comparison method was used. The relationship between VAS pain and injection satisfaction was examined by Pearson’s correlation analysis. In all analyses, the value of p <0.05 was considered as statistically significant.
Characteristics of the included patients
It was found that 60.0% of the individuals in the intervention group were female, 45.0% were in the age group of 65 years and over, 36.7% were literate, 70.0% were married, and 85.0% were unemployed. Of the individuals in the control group, 63.3% were female, 48.3% were in the age group of 65 years and over, 51.7% were literate, 78.3% were married, 88.3% were unemployed. The patients in the intervention and control groups were similar in terms of descriptive characteristics (p>0.05).
It was found that 71.7% of the patients in the intervention group did not use medications continuously, 64.7% (n=17) were using antihypertensive drugs, 71.7% had no chronic diseases other than the medical condition requiring arthroplasty, 64.7% were hypertensive patients and BMI of 48.3% of them was overweight. The mean platelet value of the patients was 279±70.80, the mean INR value was 1.00±0.14 and the mean APTT value was 23.72±2.01.
It was found that 81.7% of the patients in the control group did not use medication continuously, 45.5% (n=28) were using antihypertensive drugs, 81.7% had no chronic diseases other than the medical condition requiring arthroplasty, 54.5% had DM and BMI of 63.3% was overweight. The mean platelet value of the patients was 254±63.19, the mean INR value was 1.08±0.11, and the mean APTT value was 26.43±2.74. As a result of the analysis conducted to investigate the homogeneity of the groups, the difference between the mean platelet, INR and APTT values of the patients in the control and intervention groups was found to be statistically significant (p <0.05). The groups were similar in terms of medical properties other than the laboratory results (p>0.05).
Effect of the intervention
(Table 1) shows the distribution of VAS pain mean scores of the individuals in the intervention and control groups. While VAS pain mean score of those in the intervention group was 0.65±0.12 in the first administration, 0.76±0.10 in the second administration, and 0.70±0.89 in the third administration, this value was 0.75±0.09, 1.15±0.12, and 1.34±0.13 for the individuals in the control group, respectively. While the difference between the pain mean scores of the patients in the intervention and control group in the first administration was not statistically significant (p=0.491), the difference between the VAS pain mean scores of the intervention and control groups was found to be significantly low in the second and third administrations (p=0.019 and p=0.000) (The hypothesis H1 is confirmed).
Table 1.Distribution of VAS Pain Mean scores of the Patients in the Intervention and Control Groups
It was found that the difference between the 1st-, 2nd -, and 3rd- administration VAS pain scores of the individuals in the intervention group was not statistically significant (p=0.735). According to results of the Tamhane multiple comparison test for the individuals in the intervention group, it was observed that VAS pain level increased in the second administration but decreased in the third administration; on the other hand, the pain level in the control group increased continuously in the second and third administrations compared to the first administration and this increase was statistically significant (p=0.02).
While the injection satisfaction mean scores of the intervention groups were 9.36±0.10 in the first administration, 9.39±0.10 in the second administration, and 9.45±0.09 in the third administration, the mean scores the individuals in the control group were 8.78±0.11 (first administration), 8.74±0.13 (second administration), and 8.23±0.15 (third administration). It was found that the injection satisfaction mean scores of the intervention group were significantly higher than the mean scores of the control group and their satisfaction mean scores increased during the application (p<0.001) (Table 2).
It was determined that the injection satisfaction mean scores of the individuals in the control group decreased in the second and third administrations and the difference between them was significant (p<0.005) (Table 2).
Table 2.Distribution of Injection Satisfaction Mean Scores of the Patients in the Intervention and Control Groups
(Table 3) shows the correlation between VAS pain and injection satisfaction of the individual in the intervention and control groups during the first, second, and third administrations. A negative, statistically significant and strong correlation was found between the pain levels and injection satisfaction statuses of the patients in all three administrations (p<0.001). As the pain level experienced by the individuals due to subcutaneous injection increased, their injection satisfaction mean scores decreased.
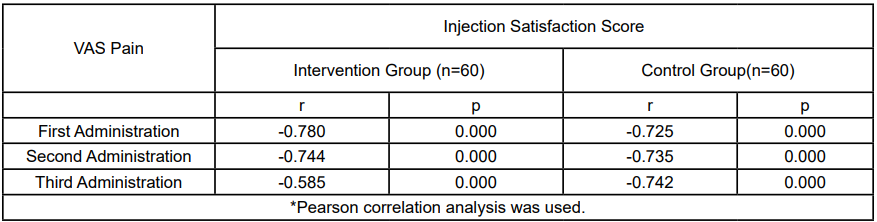
Table 3.The Correlation Between the VAS Pain and Injection Satisfaction of the Patients in the Intervention and Control Groups in the First, Second and Third Administrations
Nurses play a key role in preventing and alleviating the undesirable effects and complications of subcutaneous injections. In the present study in which we examined the effect of ShotBlocker on pain and injection satisfaction during subcutaneous injection administrations, it was determined that the pain level did not decrease in individuals in the intervention group but VAS pain mean score was significantly low in the individuals in the intervention group compared to the individuals in the control group. On the other hand, it was observed that the VAS pain level of the individuals in the control group increased statistically significantly in the 1st, 2nd, and 3rdadministrations. Based on the result of the present study, it can be said that thehypothesis H1 of “ShotBlocker is effective on pain level in subcutaneous injection administrations” is confirm. Injection technique is one of the factors causing pain development in injection site in heparin administration. In a study conducted to investigate the effect of ShotBlocker on intramuscular (IM) injection pain, IM injection procedure was performed on the patients in the application group by holding ShotBlocker during IM injection, on the patients in the placebo group by holding the reverse side of ShotBlocker (without points) on the injection site during injection and without using any tool in the control group. According to the study result, IM injection-related pain level score of the intervention group was found to be lower than the placebo and control groups (p=0.000). No difference was found between the pain level scores of the patients in the placebo and control groups [22].
In a quasi-experimental study examining the effect of “ShotBlocker” on decreasing pain due to intramuscular IM injection, intramuscular analgesic injection applied to the left ventrogluteal region of the patients constituted the experimental group; whereas, the analgesic injection applied to the right ventrogluteal regions constituted the control group.
While ShotBlocker was applied to the individuals in the experimental group by being held on the injection site during the intramuscular injection, the back side of ShotBlocker was applied to the individuals in the control group by holding it on the injection site during the injection. The pain level felt was measured using Visual Analog Scale in the first minute after the injection administration. The pain mean scores were found to be 1.22±0.62 for the experimental group and 2.48±1.12 for the control group and there was a statistically significant difference between them (p<0.001) [23].
In the study conducted by Susilawati et al., by using a tool having the same features with ShotBlocker and named as Pain-away, the newborns were divided into experimental and control groups and intramuscular Hepatitis-B vaccine was administered. The pain level of the groups was measured with DAN scale. While the pain mean scores of the experimental group was measured as 5, the pain mean scores of the control group was determined as 7 and Pain-Away was determined to be effective in reducing injection pain [27]. In the study conducted by Guevarra (2005) to reduce the pain in children during intramuscular injection, ShotBlocker was used. The mean pain level was evaluated between 0-10 in the study, the mean pain score of the experimental group was found to be 1.12 and the score of the control group was determined as 2.29. As a result of the study, injection pain of the experimental group was determined to be low compared to the control group [28]. In another study conducted with children to investigate the effect of ShotBlocker on intramuscular injection pain, it was found according to the evaluations of the nurses and caregivers that the pain scores of the children who were injected with ShotBlocker decreased but there was no difference was found according to the evaluations of the children [16].
The points placed on the surface of ShotBlocker provide stimulation for Gate Control Theory thought to exist regarding pain [9,29]. The presence and severity of pain are related to the transition of neurological stimuli. Gate mechanisms in the nervous system control the transport of pain signals. According to the Gate control theory, pain signals are carried by fibers with small diameter. Fibers with big diameters close the gate to the signals carried by fibers with small diameters. The reticular structure in the brain stem regulates sensory inputs. If sufficient or excessive sensory signals are received, the brainstem closes the gate by suppressing the transition of pain signals. If the gate is open, then the signals resulting in pain sensation reach to the consciousness level while if the gate is closed, then the stimuli do not reach the consciousness and pain is not be felt [30-32]. The proposed action mechanism of ShotBlocker is that the pressure applied on the skin by points on the tool stimulate the faster nerve ends with smaller diameters. This stimulation reduces pain by temporarily blocking slower pain signals during injection and closing gates to the central nervous system.
The pain control role of the nurse, who is the practitioner of the nursing profession established on the philosophy of comforting patients, is to keep the pain within be arable limits by knowing the pain relief approaches and to evaluate pain causes, severity, characteristics, prevalence, frequency, time and affecting factors [32,33]. Nurses play an indispensable role in the effectiveness of pain treatment and increasing patient satisfaction since they deal with patients for a longer period of time [34]. Pain related to SC injection develops due to the mechanical trauma caused by the injector insertion and the sudden pressure caused by the injection of the medication into the area. As a result of the injection-related discomfort, patients may be reluctant and dissatisfied especially about the injection applications requiring repeated dose treatments. Nurses are responsible for preventing or relieving the patient’s injection pain with the techniques they use in drug administrations. Pain management depends on the knowledge, behavior and abilities of the nurses who carry out the painful practice and is possible with the effective use of these abilities by the nurses [35].
Although the indispensability of the nurse in pain control is known, the study results and clinical observations regarding pain treatment indicate that nurses do not have sufficient knowledge and experience related to pain and are not sufficiently trained in this subject. Reducing pain associated with injection which has physical and emotional effects is important for continuance of patientnurse relationship and maintaining patient care quality and patient satisfaction [7,32].
It was determined in the present study that the use of ShotBlocker in SC injection administration increased the injection satisfaction score and the injection satisfaction mean scores of those in the intervention group were significantly higher than those in the control group (p<0.001). This result confirms the hypothesis H2. In parallel with the results of the present study, in the study by Çelik (2012) who examined the effect of ShotBlocker on reducing pain and anxiety associated with intramuscular injection, the injection satisfaction level of the intervention group was found to be higher than the placebo and control groups (p=0.000) [22]. However, no difference was determined between the satisfaction scores of the placebo and control groups. Again, in the same study, injection satisfaction mean score of the patients having injection fear was 86.7±12.73, the satisfaction mean score of the patients without injection fear was 89.5±9.27 and this difference was not statistically significant and it was determined that having fear of injection did not affect the satisfaction mean score of the patients [7].
Nurses are the primarily responsible people in relieving pain of patients and eliminating their anxiety during the presence of pain or in the practices that will cause pain. Although there are studies in the literature reporting that applications such as massage, reflexology, distraction, music therapy, buzzy technique combining cold application and vibration as well as manual pressure methods decreased injection related pain and anxiety and concern, there is almost no studies in Turkey on the applications that will relieve injection pain of adult patients [36-39]. It is an inevitable fact that nurses have an active role in relieving pain. The correct diagnosis of pain and its effective management are a prerequisite for pain control. The nurse, conducting detailed pain assessment, should select the non-pharmacological methods that can be used in pain treatment, give training to the patients about these methods, can implement it with the patient and evaluate the results in the light of such information. Nurses also have to deal with this issue and conduct practical, usable, evidence-based studies and reflect the results with proven effectiveness.
Based on the results of the present study, it was found that ShotBlocker decreased VAS pain mean score and increased the injection satisfaction, there was a negative and strong correlation between the pain level and injection satisfaction status, and ShotBlocker is an application that is easy to apply without any economic and side effects.
Based on the results of the present study, it was found that Shotblocker decreased VAS pain mean score and increased the injection satisfaction, there was a negative and strong correlation between the pain level and injection satisfaction status, and Shotblocker is an application that is easy to apply without any economic and side effects.
Since Shotblocker were applied in the study, patients knew which treatment was applied to them. Therefore, the fact that the patients included in the study knew to which group they were assigned prevented the study from being double-blind.
The authors meet the authorship criteria, and all authors are in agreement with the content of the manuscript.
The authors would like to thank all participants who participated in this study. And we would like to thank Prof. Dr. Fuat Duygulu for his contribution to the approval of the Ethics Committee and Institution.
Compliance with Ethical Standards
Before starting the application, the Academic Board permission from Erciyes University Faculty of Health Sciences, approval from Erciyes University Clinical Trials Ethics Committee (2017/400) and necessary institutional permission from the General Secretariat of Kayseri Public Hospitals were obtained. The purpose of the study was explained first and information about the study process was given to the participants by stating that their identities would be kept confidential and their written consents (Informed Consent Form) were obtained. This randomized controlled trial was performed according to the CONSORT guidelines, and registered as a clinical trial (NCT05647239).
This study is supported by the Scientific Research Project Fund of Erciyes University under project number “TYL2018-7962.”